
Discussion
E N D
Presentation Transcript
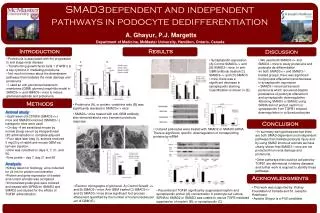
Discussion Herbert Hurwitz, MD Duke Cancer Institute Durham, NC, USA
Outline • 181: FOLFIRI +/- Panitumab: Final Results • CO.20: Cetuximab +/- Brivanib • CORRECT: BSC +/- Regorafenib
Final Results from Study 181: Randomized Phase 3 Study of FOLFIRI +/- Panitumumab for the Treatment of 2nd‑line Metastatic Colorectal Cancer A. Sobrero,1 M. Peeters,2 T. Price,3 Y. Hotko,4 A. Cervantes,5 M. Ducreux,6T. André,7 E. Chan,8 F. Lordick9 Y. Tian,10 R. Sidhu10 1Ospedale San Martino, Genoa, Italy; 2University Hospital Antwerp, Antwerp, Belgium; 3Queen Elizabeth Hospital, Woodville, Australia; 4Uzhgorod National University, Uzhgorod, Ukraine; 5Hospital Clínico, University of Valencia, Spain; 6Institut Gustave Roussy, Villejuif, France; 7Hôpital Pitié-Salpêtrière, Paris, France; 8Vanderbilt University Medical Center, Nashville, Tennessee; 9Nationales Centrum für Tumorerkrankungen, Heidelberg, Germany; 10Amgen Inc., Thousand Oaks, California
181: FOLFIRI +/- PanitumumabPFS and OS PFS OS 100 Panitumumab + FOLFIRI (n=303) Panitumumab + FOLFIRI (n=238) FOLFIRI alone (n=294) FOLFIRI alone (n=248) 80 Hazard ratio (95% CI): 0.92 (0.78, 1.10) P-value: 0.37 Hazard ratio (95% CI): 0.82 (0.69, 0.97) P-value: 0.023 60 40 20 0 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 Months Months Median (95% CI), months 6.7 (5.8, 7.4) 4.9 (3.8, 5.5) Median (95% CI), months 14.5 (13.0, 16.1) 12.5 (11.2, 14.2) Panitumumab + FOLFIRI Panitumumab + FOLFIRI FOLFIRI alone FOLFIRI alone * PFS “on treatment” HR = .73; p= .001 Adapted from: A Sobrero et al. GI Symposium 2012
181: Rash and Efficacy PFS OS 100 100 Worst ST severity 2-4 in pmab arm (n=208) Worst ST severity 2-4 in pmab arm (n=208) Worst ST severity 0-1 in pmab arm (n=83) Worst ST severity 0-1in pmab arm (n=83) 80 80 FOLFIRI alone (n=288) FOLFIRI alone (n=288) ST 2-4 vs FOLFIRI: HR=0.72; p=0.0006 ST 0-1 vs FOLFIRI: HR=1.15; p=0.28 ST 2-4 vs 0.1: HR=0.60; p=0.0003 ST 2-4 vs FOLFIRI: HR=0.80; p=0.025 ST 0-1 vs FOLFIRI: HR=1.48; p=0.003 ST 2-4 vs 0.1: HR=0.50; p<0.0001 60 60 Proportion event free (%) 40 40 20 20 0 0 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 Months Months Median (95% CI), months 7.4 (6.7, 8.5)4.0 (3.7, 5.5)5.1 (3.8, 5.5) Median (95% CI), months 16.6 (14.9, 19.4)8.4 (6.7, 11.3)12.7 (11.3, 14.3) Worst ST severity 2-4 in pmab arm Worst ST severity 2-4 in pmab arm Worst ST 0-1 severity in pmab arm Worst ST severity 0-1 in pmab arm FOLFIRI alone FOLFIRI alone Adapted from: A Sobrero et al. GI Symposium 2012
181 vs EPIC A Sobrero et al. GI Symposium 2012 A Sobrero et al. J Clin Oncol 2008. 26:2311-2319.
181: Comments • Final analyses consistent w/ primary analysis. • PFS and RR benefit, but no OS benefit • Strategies to better account for subsequent in-class treatment are needed • General PFS vs “On treatment” PFS analysis suggests treatment failure w/o progression • Rash / efficacy interaction likely important, but still not well understood • Clinical impact • Extends Panitumumab efficacy and toxicity profiles • Lack of OS benefit precludes considering P-mab/FOLFIRI as standard 2nd line option for most patients • This regimen may be appropriate for some patients 2nd line, particularly when response helpful
Phase III randomized trial of cetuximab + either brivanib alaninate or placebo in patients with metastatic, chemotherapy refractory, K-RAS wild-type colorectal carcinoma:The NCIC Clinical Trials Group and AGITG CO.20 trial LL Siu, JD Shapiro, DJ Jonker, CS Karapetis, JR Zalcberg, J Simes, F Couture, MJ Moore, TJ Price, J Siddiqui, LM Nott, D Charpentier, W Liauw, M Sawyer, M Jefford, NM Magoski, A Haydon, I Walters, D Tu, CJ O’Callaghan NCT: 00640471
Brivanib ph1b with expanded cohort in mCRC PFS (EGFR Ab naïve) Tumor response * RR 33% in EGFR Ab naive patients. M Ayers, GI Symposium 2009 CR Garrett et al BJC 2011:105, 44 – 52
CO.20 Cetuximab +/- Brivanib OS and PFS HR 0.72 (95% CI = 0.62 – 0.84) Stratified log rank p-value < 0.0001 * RR 13.6% vs 7.2% (p= .004) L Siu et al GI Symposium 2012
NCIC CTG CO.20 Grade > 3 Adverse Events L Siu et al GI Symposium 2012
NCIC CTG CO.20Effect of toxicity on compliance * Brivanib/cetuximab also had higher rates of dose reductions, missed doses, and shorter time to deterioration in quality of life. L Siu et al GI Symposium 2012
CO.20 Comments • PFS and RR benefit, but no OS benefit • OS remains primary endpoint for 3rd line mCRC • No meaningful cross over • Toxicity of combination may have confounded efficacy • Role for bFGF as a resistance mechanism for anti-VEGFR remains unknown • Potential biological antagonism remains poorly studied • Clinical impact • Unlikely to gain regulatory approval and/or significant use in combination with cetuximab • Monotherapy efficacy in mCRC is not known • Phase III HCC monotherapy trials are ongoing
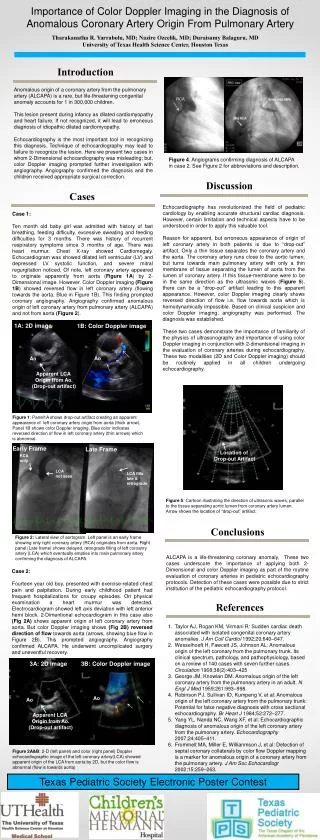
Results of a phase III randomized, double-blind, placebo-controlled, multicenter trial (CORRECT)of regorafenib plus best supportive care (BSC) versus placebo plus BSC in patients with metastatic colorectal cancer (mCRC) who have progressed after standard therapies Axel Grothey, MD Co-investigators: Alberto Sobrero, Salvatore Siena, Alfredo Falcone, Marc Ychou,Heinz-Josef Lenz, Takayuki Yoshino, Frank Cihon,Andrea Wagner, Eric Van Cutsem CORRECT: Patients with metastatic colorectal cancer treated with regorafenib or placebo after failure of standard therapy
Regorafenib and SorafenibStructure and biochemical activity Regorafenib Sorafenib SM Wilhelm, et al. Int. J. Cancer: 2011: 29, 245–255 SM Wilhelm , et al. Cancer Research 2004: 64, 7099–7109
Regorafenib metabolism Regorafenib undergoes glucuronidation and cytochrome p450 oxidation, is >99% protein bound and undergoes enterohepatic recirculation. Its M2 and M5 metabolites are bioactive. D Zopf, AACR Annual Mtg 2010, Abstr #1666
Clinical rationale for regorafenib in CRC: Phase I experience Best tumor response PFS PK for day 1 and 21 DCE-MRI changes D Strumberg ASCO 2009; Abstr # 3560
CORRECT: BSC +/- RegorafenibOS and PFS OS PFS * RR = 1.6% vs .04% A Grothey et al. GI Symposium 2012
BSC +/- Regorafenib: Safety A Grothey et al. GI Symposium 2012
CORRECT: Comments • OS and PFS Benefit • Statistically significant • Clinically meaningful for many patients • Toxicity profile significant but acceptable • Lack of cross over likely helped achieve endpoints • Clinical impact • Likely to become an available standard of care for refractory mCRC • Role in PS 2 patients not known • Role of continuous dosing not known
Why did regorafenib “work”? • Robust, randomized phase II data?– No • Robust single arm data vs consistent historical controls? – No • Ph1 mPFS = 3.3 mo; ph3 mPFS = 1.9 mo • High response rate? – No • Patient selection bio-marker? – No • Continuous dosing? – No • Activity of closely related sorafenib in refractory mCRC? – No
BAY 43-9006: RDTPatient Status at 12 Week Assessment* ** * Responses were investigator assessed ** Other Includes sarcoma, pancreas, and thyroid M Ratain, AACR-NCI-EORTC Molecular Targets and Cancer Therapeutics, , 2003
Why did regorafenib “work”? • Unique spectrum of activity – Possibly • Tie2, FGF, others TBD • PK – Probably • Role of M2 and M5 metabolites? • Clean phase III study design – Probably • No cross over, no chemo to confound efficacy or toxicity, mature therapeutic class • Value of the VEGF target - Probably • Bevacizumab • 1st /2nd line PFS/OS, 1-10% RR as monotherapy; “Bev Beyond Progression” OS HR = .52; 3rd line TRC103: RR 1-4%, PFS 3.5mo, OS 9.0mo. • Aflibercept 2nd line OS HR = .82 • Multiple VEGF TKIs have shown biological activity but only borderline clinical efficacy in combination with chemotherapy • But no randomized studies of monotherapy vs BSC H Hurwitz NEJM 2004. 350:2335-2342. B Giantonio JCO 2007 .25 : (12) 1539-1544. F Kabbinavar JCO 2003. 21: (1) 60-65. L Saltz JCO 2008 . 26 :(12) 2013-2019. A Grothey ECCO-ESMO2011. H Chen JCO 2006.24 :(21)3354-3360. E Van Cutsem, ESMO/WCGIC 2011. Abstract O-0024 J Tabernero et al. ECCO-ESMO 2011.
Overall Conclusions • Three excellent studies by excellent teams • Regorafenib will likely join the list of useful therapeutics for mCRC • Efforts to improve its efficacy are still needed • Biomarker candidates have been suggested by many groups • Efforts to improve regorafenib’s toxicity profile are also needed • Risk/benefit in PS2 patients not yet known • 181 and CO.20 were only “borderline” negative studies • Why? • Trial design, tolerability, and sustainability still matter • Rushing from phase I to phase III can work, but be careful • Agents for novel targets beyond VEGF and EGFR are needed • mCRC is an excellent disease setting to test these agents