Case Management: Acute Respiratory Failure
710 likes | 913 Vues
Case Management: Acute Respiratory Failure. Santos, Jennifer Joy Santos, Ma. Socorro Tiongson , Denver. Y.d. 57 year old Female Widow Born Again Christian Right-handed from Baclaran , Paranaque. Patient Profile. Chief Complaint : Dyspnea

Case Management: Acute Respiratory Failure
E N D
Presentation Transcript
Case Management:Acute Respiratory Failure Santos, Jennifer Joy Santos, Ma. Socorro Tiongson, Denver
Y.d. • 57 year old • Female • Widow • Born Again Christian • Right-handed • from Baclaran, Paranaque
Patient Profile • Chief Complaint : Dyspnea • Non-hypertensive, non-diabetic, non-asthmatic • No history of PTB • With a finding of an intracranial mass (temporal lobe) in CT scan c/o PGH (2005)
Family history • (+) HPN- mother • (+) CVD- siblings • (+) MI- brother • (-) known Cancer of any type • (-) PTB, DM
Personal /social history • Non-smoker • Non alcoholic beverages • Denies illicit drug use • Works in buy and sell business • Church worship leader • High school graduate • Lives with youngest daughter aged 16 y/o in their old house, while the other 2 daughters are now living with their respective families
PBS: normocytic, hypochromic (++), (+) toxic granulation in PMNs. Reticulocytes adequate.
PTB extensive disease with possible cavitation Pneumonia with consolidation Subsegmentalatelectasis, L • WAT IS OUR aditional READING of this XRAY? • Elevated Right diaphragm can mean pulmonary contraction • - cardiac reading?
Other pertinent laboratory results 3/11 • ETA GS: 0-2 gram (-) bacilli; 0-2 yeast cells • KAYA KAYA NATING MAHANAP YUNG CULTURE STUDIES NYA PARA MALAMAN UNG ETIOLOGIC AGENT? =)
Physical examination on admission • Awake, conscious, responsive, intubated @ET 7.5 L18, NICRD • BP= 120/80 HR=120 RR=40s T=37.6 • HEENT: pale palpebral conjunctivae, anictericsclerae, pupils 2mm EBRTL, (+) NVE, (+) Anterior neck mass 3x4 cm firm, nodular, movable. (-) CLAD • Chest: Equal chest expansion, harsh breath sounds, (+) crackles bilateral LF mid to base, (-) wheezes. • Heart: DHS, tachycardic, regular rhythm, apex beat at 5th ICS anterior axillary line. (-) murmurs. • Abdomen: soft, flabby, normoactive bowel sounds, (-) masses/tenderness • Extremities: pink nailbeds, full and equal pulses, CRT<2 sec. (-) edema/cyanosis, (+) grade I sacral ulcer, Right
Other pertinent laboratory findings 3/12 • CKMB 23.5 • CK total 42 Rules out ACS
3/11/2010, 9 AM Course in the ward • noted BP 70/50 • A> ARDS 2’ CAP HR • Sepsis secondary to CAP HR • PTB cat I • Intracranial mass, R lobe • DTG in storm, s/p RAI • IFG • Dyslipidemia • Anemia prob secondary to chronic disease. • Dopamine drip started
3/12 : 12-L ECG: MFAT, normal axis, non-specific ST-T wave changes
Sinus tachycardia, normal axis, low voltage complexes, NSSTTWC
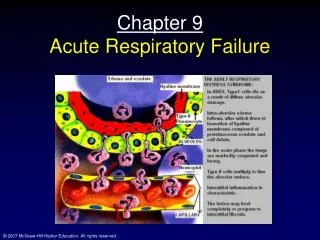
ARDS • Severe dyspnea of acute onset (< 2 weeks) • Hypoxemia • Diffuse bilateral pulmonary infiltrate on CXR • PaO2/FiO2 < 200 mmHg • No elevated left atrial pressure (PCWP <18 mm Hg) • Respiratory • Failure
Three Phases Recovery Exudative Proliferative Fibrotic 0 7 14 21 6 mos
Diffuse alveolar and endothelial damage Increase pulmonary vascular permeability Atelectasis and increase work of breathing: Dyspnea Tachypnea Hypoxemia Microvascular occlusion, pulmonary hypertension, increase in dead space: Hypercapnia Alveolar edema PMN infiltration of lungs Hyaline membrane formation Inactivation of surfactant due to exudates Accumulation in dependent portions Atelectasis
Proliferative Phase • Time of Lung repair • Layering of exudates • Lymphocytic infiltration • Type II pneumocytes reproduce surfactant
Fibrotic Phase • Fibrosis • Emphysema like changes (bullae) • Vascular occlusion • Complications: • Pulmonary Hypertension • Pneumothorax • Increase in dead space
Mechanical Ventilation • Augments the increase in work of breathing • But can aggravate lung injury via repeated Alveolar Overdistention and Recurrent Alveolar Collapse • Set MV at lower tidal volumes • 6 ml/kgBW( vs standard 12ml/kgBW) • Optimal PEEP for alveolar recruitment : • 12-15 cmHg • Target RR < 35 • ARDS net protocol: Low volume, High frequency ventilation
Management • Manage Respiratory Acidosis • Fluid restriction and diuretic • to reduce left atrial filling pressure • Dry Lungs are Happy Lungs! • Steroids • anti-inflammatory No role!
Mortality • 41-65% • Mostly from non-pulmonary causes (Sepsis, organ failure) • Recovery of lung function within 6 months
Inability of the lung to meet the metabolic demands of the body • Dysfunction in lung’s main function: • Oxygenation • Carbon Dioxide elimination • PaO2 <60 mmHg • PaCO2 >50 mmHg • Develops 4-48 hours
Signs • Tachypnea • Exaggerated use of accessory muscles • Intercostal, supraclavicular and subcostal retractions • Neuromuscular disease: signs of respiratory distress may not be obvious • CNS disease: bradypnea + shallow breathing