Download
1 / 25
250 likes | 441 Vues
Part of a mini-symposium presented at the Annual Meeting of the American College of Sports Medicine in Baltimore, May 31, 2001. Client Assessment and Other New Uses of Reliability. Reliability: the Essentials Assessment of Individual Clients and Patients

E N D
Part of a mini-symposium presented at the Annual Meetingof the American College of Sports Medicine in Baltimore,May 31, 2001 Client Assessment and Other New Uses of Reliability • Reliability: the Essentials • Assessment of Individual Clients and Patients • Estimation of Sample Size for Experiments • Estimation of Individual Responses to a Treatment Will G HopkinsPhysiology and Physical EducationUniversity of Otago, Dunedin NZ
Reliability: the Essentials • Reliability is reproducibility of a measurement if or when you repeat the measurement. • It's crucial for clinicians…because you need good reproducibility to monitor small but clinically important changes in an individual patient or client. • It's crucial for researchers…because you need good reproducibility to quantify such changes in controlled trials with samples of reasonable size.
Subject Trial 1 Trial 2 Trial 3 Trial 4 Trial 5 Trial 6 Mean ± SD Chris 72 76 74 79 79 77 76.2 ± 2.8 Reliability: the Essentials • How do we quantify reliability? • Easy to understand for one subject tested many times: • The 2.8 is the standard error of measurement. • I call it the typical error, because it's the typical difference between the subject's true value and the observed values. • It's the random error or noise in our assessment of clients and in our experimental studies. • Strictly, this standard deviation of a subject's values is the total error of measurement.
Subject Trial 1 Trial 2 Trial 2-1 Chris 72 76 4 Jo 53 58 0 Kelly 60 60 -2 Pat 84 82 6 Sam 67 73 2.6±3.4 Mean ± SD: Reliability: the Essentials • We usually measure reliability with many subjects tested a few times: 5 • The 3.4 divided by 2 is the typical error. • The 3.4 multiplied by ±1.96 are the limits of agreement. • The 2.6 is the change in the mean.
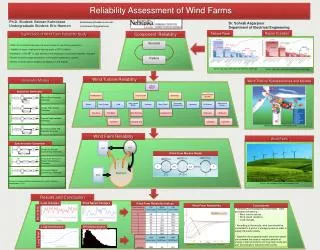
90 Pearson r = 0.96 Trial 2 70 Intraclass r = 0.95 50 50 70 90 Trial 1 Reliability: the Essentials • And we can define retest correlations:Pearson (for two trials) and intraclass (two or more trials).
Assessment of Individual Clients and Patients • When you test or retest an individual, take account of relative magnitudes of signal and noise. • The signal is what you are trying to measure. • It's the smallest clinically or practically important change (within the individual) or difference (between two individuals or between an individual and a criterion value). • Rarely it's larger changes or differences.
Assessment of Individual Clients and Patients • The noise is the typical error of measurement. • It needs to come from a reliability study in which there are no real changes in the subjects. • Or in which any real changes are the same for all subjects. • Otherwise the estimate of the noise will be too large. • Time between tests is therefore as short as necessary. • A practice trial may be important, to avoid real changes. • If published error is not relevant to your situation, do your own reliability study.
Assessment of Individual Clients and Patients • If noise << signal... • Example: body mass; noise in scales = 0.1 kg, signal = 1 kg. • The scales are effectively noise-free. • Accept the measurement without worry. • If noise >> signal... • Example: speed at ventilatory threshold; noise = 3%, signal = 1%. • The noise swamps all but large changes or differences. • Find a better test.
Assessment of Individual Clients and Patients • If noise signal... • Examples: many lab and field tests. • Accept the result of the test cautiously. • Or improve assessment by... 1. averaging several tests 2. using confidence limits 3. using likelihoods 4. possibly using Bayesian adjustment
Assessment of Individual Clients and Patients 1. Average several tests to reduce the noise. • Noise reduces by a factor of 1/n, where n = number of tests. 2. Use likely (confidence) limits for the subject's true value. • Practically useful confidence is less than the 95%of research. • For a single test, single score ± typical errorare 68% confidence limits. • For test and retest, change score ± typical error are 52% confidence limits.
If you see a change of 1.5, -0.9 0.9 the true change is 52% likely to be between 0.5 and 2.5. negative trivial positive If you see a change of 0.5, the true change is 52% likely to be between -0.5 and 1.5. -2 -1 0 1 2 Change score Assessment of Individual Clients and Patients • Example of likely limits for a change score: noise (typical error) = 1.0, smallest important change = 0.9. "a positive change?" "no real change?"
Assessment of Individual Clients and Patients 3. Use likelihoods that the true value is greater/less than an important reference value or values. • More precise than confidence limits, but needs a spreadsheet for the calculations. • For single scores, the reference value is usually a pass-fail threshold. • For change scores, the best reference values are ± the smallest important change.
If you see 1.5, chances are... -0.9 0.9 66% the true change is positive; 29% the true change is trivial; negative trivial positive 5% the true change is negative. 66% 5% 29% 16% 45% 39% If you see 0.5, chances are...39% the true change is positive;45% the true change is trivial;16% the true change is negative. -2 -1 0 1 2 Change score Assessment of Individual Clients and Patients • Same example of a change score, to illustrate likelihoods: noise (typical error) = 1.0, smallest important change = 0.9. "a positive change" "maybe no real change"
Assessment of Individual Clients and Patients 4. Go Bayesian? • That is, take into account your prior belief about the likely outcome of the test. • When you scale down or reject outright an unlikely high score, you are being a Bayesian... • because you attribute the high score partly or entirely to noise, not the client.
Assessment of Individual Clients and Patients • To go Bayesian quantitatively… • 1. specify your prior belief with likely limits; • 2. combine your belief with the observed score and the noise to give… • 3. an adjusted score with adjusted likely limits or likelihoods. • But how do you specify your prior belief believably? • Example: if you believe a change couldn't be outside ±3, where does the ±3 come from, and what likely limits define couldn't? 80%, 90%, 95%, 99%... ? • So use Bayes qualitatively but not quantitatively.
Estimation of Sample Size for Experiments • Based on havingacceptable precision for the effect. • Precision is defined by 95% likely limits. • Estimate of likely limits needs typical error from a reliability study in which the time frame is the same as in the experiment. • If published error is not relevant, try to do your own reliability study. • Acceptablelimits…
negative trivial positive Therefore 95% likely limits = smallest important effect= ± d -d d 0 Effect (change score) Estimation of Sample Size for Experiments • Acceptablelimits can't be both substantially positive and negative, in the worst case of observed effect = 0. • For a crossover, 95% likely limits =±[2 x (typical error)/(sample size)] xt0.975,DF = ± d, where DF is the degrees of freedom in the experiment. • Therefore sample size ≈ 8(typical error)2/d2, so...
Estimation of Sample Size for Experiments • When typical error ≈ smallest effect, sample size ≈ 8. • For a study with a control group, sample size ≈ 32(4x as many). • Beware: typical error in an experiment is often larger than in a reliability study, so you may need more subjects. • When typical error << smallest effect, sample size could be ~1, but use ~8 in each group to ensure sample is representative.
Estimation of Sample Size for Experiments • When typical error >> smallest effect… • Test 100s of subjects to estimate small effects. • Or test fewer subjects many times pre and post the treatment. • Or use a smaller sample and find a test with a smaller typical error. • Or use a smaller sample and hope for a large effect. • Because larger effects need less precision. • If you get a small effect, tell the editor your study will contribute to a meta-analysis.
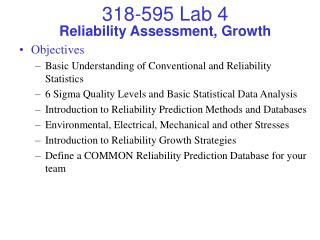
same reliability different reliability No IndividualResponses to Drug Substantial IndividualResponses to Drug placebo drug placebo drug 80 testscore 60 40 pre post pre post pre pre post post time time Individual Responses to a Treatment • An important but neglected aspect of research. • How to see them? Three ways. 1. Display each subject's values:
relatively larger Each subject'svalues Means andstandard deviations placebo drug 80 80 drug testscore testscore 60 60 40 40 placebo pre pre post pre post post time time Individual Responses to a Treatment 2. Look for an increase in the standard deviation of the treatment group in the post test. • But you might miss it:
Each subject'svalues Means and SDsof change scores 30 placebo drug 80 testscore post-prescore 20 60 10 40 0 pre post pre post placebo drug Individual Responses to a Treatment 3. Look for a bigger standard deviation of the post-pre change scores in the treatment group. • Now much easier to see any individual responses: • To present the magnitude of individual responses...
Individual Responses to a Treatment • Express individual responses as a standard deviation. • Example: effect of drug = 14 ± 7 units (mean ± SD). • This SD for individual responses is free of measurement error. • It is NOT the SD of the change scorefor the drug group. • There is a simple formula for this SD (see next slide), but getting its likely limits is more challenging. • If you find individual responses, try to account for them in your analysis using subject characteristics as covariates.
Individual Responses to a Treatment • How to derive this standard deviation: • From the standard deviations of the change scores of the treatment and control groups: (SD2treat-SD2cont). • Or from analysis of the treatment and control groups as reliability studies: 2(error2treat-error2cont). • Or by using mixed modeling, especially to get its confidence limits. • Identify subject characteristicsresponsible for the individual responses by using repeated-measures analysis of covariance. • This approach also increases precision of the estimate of the mean effect.
This presentation, spreadsheets, more information at: A New View of Statistics newstats.org SUMMARIZING DATA GENERALIZING TO A POPULATION Simple & Effect Statistics Precision of Measurement Confidence Limits Statistical Models Dimension Reduction Sample-Size Estimation