RENAL REPLACEMENT THERAPY (RRT)
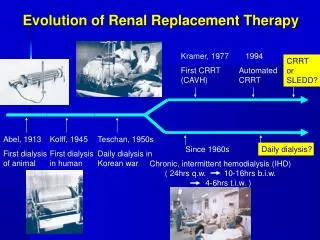
RENAL REPLACEMENT THERAPY (RRT). RRT: Modalities. Hemodialysis Peritoneal Dialysis Renal Transplantation Living-Related, Living-Unrelated Cadaveric CRRT CAVH, CVVH, SCUF CAVHD,CVVHD, CAVHDF, CVVHDF. RRT: Absolute Indications for Dialysis. Fluid Overload

RENAL REPLACEMENT THERAPY (RRT)
E N D
Presentation Transcript
RRT: Modalities • Hemodialysis • Peritoneal Dialysis • Renal Transplantation • Living-Related, Living-Unrelated • Cadaveric • CRRT • CAVH, CVVH, SCUF • CAVHD,CVVHD, CAVHDF, CVVHDF
RRT: Absolute Indications for Dialysis • Fluid Overload • Hyperkalemia • Severe Metabolic Acidosis • Uremic Pericarditis • Uremic Enchephalopathy • Intoxication: Methanol, ethylene glycol ASA, & Lithium
RRT: Relative Indications for Dialysis • Uremic Neuropathy • Malnutrition of CRF • Correct bleeding time before surgery • Cr. clearance <10 ml/minute • Level of urea & creatinine ??
Hemodialysis: Dialyzer Arterial blood from Patient out going dialysate Incoming Dialysate solution Venous blood to patient
Hemodialysis: Principles • Solutes are effectively removed by diffusion • Water is removed by convection (UF) • Both mechanisms contribute to solute removal
Peritoneal Dialysis: Types • Continuos Ambulatory Peritoneal Dialysis (CAPD) • 4 cycles of 2 liter of dialysate • Intermittent Peritoneal Dialysis (IPD) • Whole day or night for 2-3 times/ week • Continuos Cyclic Peritoneal Dialysis (CCPD) • Eight , 2 liters exchanges during night
Peritoneal Dialysis: Principle • Diffusion: for solutes • From high concentration gradient to low concentration gradient • Osmosis: for water • Depends on concentration of sugar in the dialysate fluid • The fluid and solute removal can be enhanced by increasing the volume of dialysate and the number of exchanges
Peritoneal Dialysis: CAPD, IPD Hanger PD dialysate solution Connection set PD Catheter draining bag
PD: Advantages • A more normal life-style • Better residual renal function • Less stringent fluid and diet restriction • Stable solutes concentration (no dysequilibrium) • Better hemoglobin level • More economic: 2/3 of HD cost
PD: Complications • CAPD PERITONITIS • Abdominal pain • Fever • Turbid effluent • WBC in effluent >400 • Organisms: • Staph. aureus and epidermedis • Gram negative: Klebseilla, pseudomonas • Candida
CAPD PERITONITIS: Treatment • 3 flushes in & out • Loading dose Intraperitoneal antibiotics: • Cefazoline and Tobramycin Or • Vancomycin & Tobramycin • Maintenance dose IP antibiotics: • Change antibiotics according to sensitivity
CAPD: Complications & Treat. • Tunnel infection • Pain and swelling at tunnel site • Fever • Treatment: Vancomycin IV • Exit site infection • Redness at exit site with discharge • Cloxacillin or Vancomycin
CAPD: Complications & Treat. • Catheter leak • Treatment: Temporary conversion to HD • Catheter dysfunction: causes • Constipation: laxatives • Fibrin: IP heparin • Omental wrap • May require replacement
CAPD: Complications • Obesity & hypertriglyceridemia • Due to excessive absorption of glucose • Protein loss & hypoalbuminemia • Loss with the effluent • Bloody Effluent: • Ruptured corpus leutium (ovulation) • Endometriosis
CRRT: Types • CAVH: UF only • CVVH: UF only • SCUF: slow UF • CAVHD: Dialysis • CVVHD: Dialysis • CAVHDF: UF & Dialysis • CVVHDF: UF & Dialysis
CRRT: Principle • Ultrafiltration: The main driving force • Diffusion: slow and efficient only with time • Patient need replacement of fluid loss up to 18 liters/ day (in CAVH, CVVH, CAVHDF & CVVHDF)
CRRT: CAVH Replacement Arterial Venous Qb=50-100 ml/min Qf= 8-12 ml/min UF
CRRT: CAVHD Dialysate In Arterial Venous Qb=50-100 ml/min Qd=10-20 ml/min Qf= 1-3 ml/min Dialysate out
CRRT: CVVH Replacement Venous Venous Pump Qb=50-200 ml/min Qf= 10-20 ml/min UF
CRRT: CVVHD Dialysate In Pump Venous Venous Qb=50-200 ml/min Qd=10-30 ml/min Qf= 1-5 ml/min Dialysate out
CRRT: Indications • Acute Renal failure in hemodynamically unstable patient & MOF • Volume control in septic patient with no Renal failure • Removal of mediators of sepsis • Refractory Congestive Heart Failure • ARF in acute and chronic liver disease • Tumor lysis syndrome, lithium intox.?