Adrenal Incidentaloma
840 likes | 2.84k Vues
Adrenal Incidentaloma. Adrenal Incidentaloma. Adrenal mass detected during abdominal imaging done for other reasons. Autopsy series - adrenal masses in 1.4 - 9% Noted in 5% of patients who undergo CT scans. The Adrenal Gland. The Adrenal Gland.

Adrenal Incidentaloma
E N D
Presentation Transcript
Adrenal Incidentaloma • Adrenal mass detected during abdominal imaging done for other reasons. • Autopsy series - adrenal masses in 1.4 - 9% • Noted in 5% of patients who undergo CT scans
Differential Diagnosis of Adrenal Incidentalomas • Cortical Adenoma • Cysts • Hemorrhage • Myelipoma • Pheochromcytoma • Gnaglioneuroma • Adrenal Carcinoma • Metastatic Cancer • Granulomatosis • Tuberculosis • histoplasmosis, • blastomycosis • Abscess • Amyloidosis • Fibroma
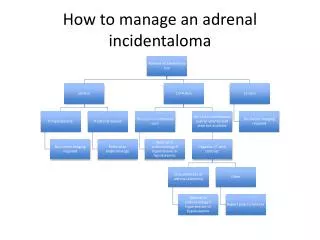
Two main questions when working up an Incidentaloma Is it a Functioning Mass? Is it a carcinoma?
Is it a Functioning Mass? • Aldosterone • Cortisol • DHEAS • Pheochromocytoma
Patient presents with hypertension and hypokalemia. Found to have a 1.3 cm left adrenal mass. Further workup revealed a high serum aldosterone and a low serum renin. What is this consistent with ? Aldosterone secreting adrenal adenoma (Conn's syndrome).
Hyperaldosteronism • Symptoms are often non specific • Hypokalemia • weakness, cramps, polyuria • Hypertension • may be severe and refractory to treatment • Metabolic alkalosis
Primary hyperaldosteronism • Subtypes of primary Aldosteronism • Aldosterone producing adenoma • Idiopathic hyperaldosteronism • Primary adrenal hyperplasia • Aldosterone producing adrenocortical carcinoma • Aldosterone producing ovarian tumor • Familial hyperaldosteronism
Random PRA and PAC Random PRA and PAC PA = Primary Aldosteronism
Primary Aldsteronism • If adrenal mass is > 1 cm proceed with adrenalectomy • If mass is < 1 cm, then recommend adrenal vein sampling • if lateralises then adrenalectomy • if not - ? Idiopathic hyperaldosteronism
Is it a functioning mass? Cortisol What is Cushing’s Syndrome? • Hypercortisolism • ACTH dependent • pituitary cushing’s • ectopic ACTH • ACTH independent ( 20% ) • adrenal adenoma/carcinoma/hyperplasia • iatrogenic List some features of the syndrome ! Truncal obesity Gonadal dysfunction Hirsutism/Acne Muscle weakness Facial fullness Glucose intolerance Skin atrophy/bruising Edema
Cushing’s Syndrome • Really Subclinical Cushing’s • Rarely progresses to overt Cushing’s • Found in mean rate of adrenal incidentalomas 8% • Incidentalomas < 1cm do not need w/u for Cushing’s • since hypercortisolism extremely rare
Low Dose Dexamethasone Suppression Test • Day 1 • at 0900 take fasting blood cortisol • Immediately inject 0.5mg Dexamethasone • Give further 0.5mg at 1500,2100 and 0300 hrs • Day 2 • at 0900 take fasting blood cortisol • Immediately inject 0.5mg Dexamethasone • Give further 0.5mg at 1500,2100 and 0300 hrs • Day 3 • at 0900 take fasting blood cortisol The High Dose Test is the same using 2mg
Cushing’s Syndrome caused by adrenal tumor • low dose: no change • high dose:no change • Cushing’s Disease • low dose: no change • high dose: normal suppression • Cushing’s Syndrome caused by ectopic ACTH • low dose: no change • high dose:no change
Is it a functioning mass ? • DHEAS - Dehydroepiandrosterone sulfate • secreted directly and almost exclusively by the adrenal Signs of Virilization in women ! • hirsutism • temporal balding • voice changes • clitoral enlargement • acne • increased muscle mass • decreased breast size • amenorrhea
Before we proceed……. chromaffin 1.The medulla is composed of ____________ cells derived from the_____________. neural crest. 2.Most extra-adrenal pheochromocytomas are located at the ______________ Organ of Zuckerkandl the bladder 3.Patients with pheochromocytomas in ____________wall may present with __________ loss of consciousness due to catecholamine release. post-voiding
Pheochromocytoma • Secrete both epi and norepinephrine • < 0.1% of hypertensive patients • 85 - 90% - Adrenal Medulla • MEN - multiple endocrine neoplasia • Type II A - medullary CA, parathyroid • Type II B - medullary CA, neuromas, marfanoid Rule of 10 Familial malignant extra-adrenal. malignant sporadic bilateral
Complications of pheochromocytoma crisis • shock • DIC • seizures • rhabdomyolysis • acute renal failure • death.
Pheochromocytoma Work up Labs: Electrolytes 24 hr urine metanephrines Plasma catecholamines Ann Int Med (2001)134:315-329 • Urinary metanephrines above 1.2 mg/day (6.5 µmol/day) • false-positive results can very rarely occur • labetalol • buspirone • caffeine
Imaging for Pheochromocytoma CT and MRI have higher sensitivity than 131I-MIBG However, 131I-MIBG uptake is more specific Some authors prefer to use MIBG as the initial screening modality because it enables whole-body imaging makes it useful for detection of extra-adrenal tumors and metastatic deposits. the false-negative rate of MIBG scintigraphy is 10%. CT/MRI still done CT - quick/relatively inexpensive but not specific enough to distinguish masses hypertensive crisis after the injection of contrast material - reported MRI - more specific than CT, but some patients cannot tolerate MRI.
Is it Malignant? • Pt’s with known malignancy • 8 -38% pts with known malignancy • have adrenal mets at autopsy • Most common primary • breast • lung • kidney • melanoma • lympoma • CT guided FNA may be of value
Adrenocortical carcinoma - 0.5/million - incidence • 5 year survival • localized disease:70% • metastases:5.3%
Imaging: favoring benign Small size Round regular shape homogeneity low density on CT low T2 weighted signal high lipid content Imaging: favoring malignant Large size ( >5cm ) irregular shape heterogeneity high density on CT high T2 weighted signal low lipid content demonstratable growth
SIZE - it does matter ! • The probability of malignancy increases with size • At a cut off of 4cm, the mal/benign ratio - 8:1 • Recommendations - remove all lesions > 4 cm