Download
1 / 25
250 likes | 1.62k Vues
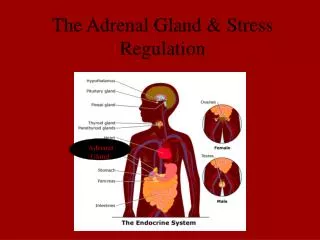
Adrenal Incidentaloma: An Update of its Management. 18 th September 2004. Dominic Tai Division of Urology Department of Surgery Pamela Youde Nethersole Eastern Hospital. Agenda. Prevalence and pathologies Diagnostic Evaluation Risk of malignancy Hormonal evaluation Imaging

E N D
Adrenal Incidentaloma:An Update of its Management 18th September 2004 Dominic Tai Division of Urology Department of Surgery Pamela Youde Nethersole Eastern Hospital
Agenda • Prevalence and pathologies • Diagnostic Evaluation • Risk of malignancy • Hormonal evaluation • Imaging • Surgical options • Take home messages
Definition • Clinically silent adrenal mass • Incidentally discovered by imaging performed for unrelated problems
Prevalence • Autopsy series of more than 8500 patients from 25 series: • 5.9% (1-32%) • CT: • 0.6-1.9% • Data obtained >10 yrs ago (thick cut CT 5mm-1cm) • Prevalence increases with age • <30 less than 1% • Middle age 3% • Elderly>70 10% • Kloos RT et al: Incidental discovered adrenal masses. Endocrine Rev 1995, 16:460-484
Pathology F. Mantero et al J. Clinical Endocrinol Metab 85:637-644, 2000 -
Diagnostic Evaluation • Assessment of risk of malignancy • Primary • Secondary • Hormonal evaluation • Subclinical endocrine activity is not uncommon in asymptomatic patients
Adrenocortical Carcinoma • Rare but lethal tumor • Overall 5 yr survival ~ 16% • For small tumor confined to adrenal gland ~42% • Major indicator of malignancy • Size • Other features for adrenal malignancy in CT: • Density >18 HU • Irregular tumor margin • Heterogeneity/hemorrhage/necrosis • Lymphadenopathy/invasion to adjacent organs
Distribution of diagnosis by tumor size(8 studies with 103 diagnoses determined by histology)
Recommendation for Non-functioning Adrenal Incidentaloma • High risk patients surgical removal • Tumor size >6cm • Features of malignancy in imaging studies • Low risk patients Follow-up • Tumor size <4 cm • Medium risk patients both approach reasonable • Tumor size between 4-6 cm
Adrenal Metastasis • Frequent site for metastasis • 27% in 1000 consecutive autopsies of cancer patients • Incidence approaching 40% in patients with CA lung • Abrams HL et al. Cancer 3:74-85. 1950 • Metachronous isolated metastasis • Adrenalectomy may prolong median survival • Cord Sturgeon et al. Surgical clinics of North America. 84:2004
Fine needle Aspiration • Little role in differentiating different pathologies • Potentially serious complications • Concerns of track seeding • Sampling error • Negative biopsy unable to rule out malignancy • Inconclusive biopsy results may happen • Useful in evaluation of suspicious adrenal secondary • Important to rule out phaeochromocytoma first before attempting biopsy • Potentially life threatening hypertensive crisis
Incidence of SubclinicalEndocrine Activities • Hypercortisolism: 5-47% • Hyperaldosteronism: 1.6-3.8% • Phaeochromocytoma: 7-10% • Sex hormone secreting tumor: rare • George Mansmann et al. Endocrine Review25(2): 309-340
Hormonal EvaluationSubclinical Cushing Syn(Subclinical Autonomous Glucocorticoid Hypersecretion) • Symptoms and signs not apparent and specific • Screening • Low dose dexamethasone (1mg) suppression test • NIH State of Science Recommendation • Confirmation • High dose dexamethasone suppression • ACTH • 24 hr urine free cortisol
Hormonal EvaluationPhaeochromocytoma • Endocrine test advised in all incidentalomas • (including normotensive ones) • 24 hr urinary free catecholamines • its metabolites • VMA and metanephrines • Plasma free catecholamine metabolites (?more sensitive) • NIH State of Science Recommendation
Hormonal EvaluationPrimary Aldosteronism • Screening advised • Even patient normokalaemic • Screening test • Aldosterone/plasma renin activity • NIH State of Science Recommendation • Lateralization • CT/MRI • Scintigraphy • Adrenal vein sampling
Imaging studies • CT • Still remain an accurate tool • 97-99% sensitivity (spiral thin cut) • Solitary lesion >1cm with normal contralateral gland • Adrenal limb thickness • Lingam et al AJR 2003;181(3): 843-9 • MRI • Inconclusive results when compared with CT • May be slightly more sensitive to differentiate the pathology • Very sensitive in detecting phaeochromocytoma • (light bulb appearance on T2 images) • Useful for staging for advanced carcinoma • Georg et al Endocrin Review 2004;25(2) 309-340
Imaging StudiesUSG • Less sensitive than CT and MRI • For adrenal tumor < 3cm • Missed 35% of lesion • Almost 100% were detected by CT • Suzuki K et al. J. Urol 154: 484-486 1995 • Operator dependent • Limited role for diagnosis and Follow-up
Imaging StudiesScintigraphy • NP-59 • Role in differentiation • Hyperplasia/adenoma • Use in incidentaloma controversial • MIBG • Only indicated for suspected malignant/ familial case
Indication for adrenalectomy • Suspicion for malignancy • Mass with hormonal hypersecretion
Adrenalectomy European Association of Urology Guideline 2002 Laparoscopic Superior to Open • Expert opinion : Superior • Level of evidence : 1b • Recommendation : Grade A
Contraindications • Invasive cortical carcinoma • Adjacent organ/major vessel invasion • Regional lymphadenopathy • Solitary adrenal metastasis • Can be safely managed by Lap adrenalectomy • Obesity and history of abdominal operation • No more contraindicated
Take Home Messages • Adrenal incidentaloma requires • Hormonal evaluation • Assessment for risk of malignancy • Risk of malignancy is mainly determined by its size • Laparoscopic adrenalectomy is the gold standard for adrenal gland removal • Except in invasive malignancy