Download
1 / 53
540 likes | 929 Vues
Adrenal Steroid Hormones. Review of the Adrenal Gland Review of Adrenal Steroidogenesis The Adrenal Medulla Production and Roles of Cortisol Production and Roles of Aldosterone Adrenal Androgens. Adrenal Steroids: A Review.

E N D
Adrenal Steroid Hormones Review of the Adrenal Gland Review of Adrenal Steroidogenesis The Adrenal Medulla Production and Roles of Cortisol Production and Roles of Aldosterone Adrenal Androgens
Adrenal Steroids: A Review • The adrenal glands are located immediately superior to the kidneys. • There are three classes of adrenal steroids: • - mineralocorticoids, • - glucocorticoids, and • - androgens
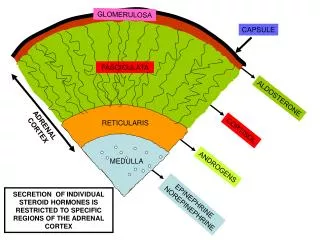
Organization of the Adrenal Gland There is an adrenal cortex and adrenal medulla. Steroids are made in the 3 zones of the adrenal cortex: mineralocorticoids: zona glomerulosa glucocorticoids: zona fasciculata androgens: zona reticularis
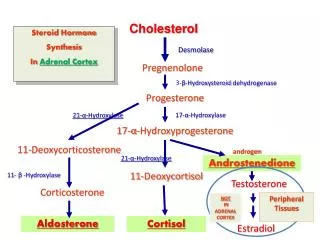
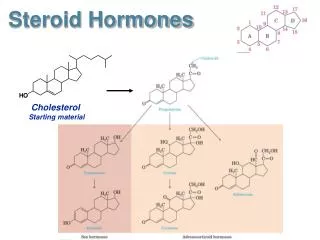
Adrenal Steroidogenesis • The first step is the conversion of cholesterol to pregnenolone, which occurs in the mitochondria. • This reaction is carried out by the enzyme, cytochrome P450 side chain cleavage (P450scc). • This is a rate limiting, nonreversible enzymatic step in the initiation of steroid biosynthesis.
17a-hydroxylase lyase pregnenolone 17a-hydroxypregnenolone dehydroepiandrosterone progesterone androstenedione glucocorticoids mineralocorticoids (cortisol) (aldosterone) 3b-hydroxysteroid dehydrogenase 21-hydroxylase 11 b-hydroxylase 18 hydroxylase/oxidase Adrenal Steroidogenesis • Next, pregnenolone can be converted (in smooth ER) into three different pathways, depending upon whether you want to make mineralcorticoids, glucocorticoids, or androgens:
Adrenal Steroidogenesis • What determines which pathway is taken? • Each step of the pathway is regulated by a specific enzyme. • Different zones of the adrenal cortex have different relative activities of enzymes, resulting in different chemical reactions taking place. • These enzymes are located in the smooth ER. • Earlier in this course, you did not have to learn the names of these enzymes. Now, with your advanced understanding, you do!
What about the Adrenal Medulla? • While the adrenal cortex is derived from mesoderm, the adrenal medulla is derived from neural crest cells, and is referred to as chromaffin tissue. • Produces epinephrine (80%) and norepinephrine (20%), derived from tyrosine. • Synthesis of epinephrine requires cortisol. • Medulla also contains some steroidogenic enzymes, may contribute to completion of steroid production.
Ach epinephrine calcium Regulation of Epinephrine Release • Released in response to preganglionic sympathetic stimulation. • Preganglionic fibers release acetylcholine. • Acetylcholine binds to nicotinic receptors on chromaffin cells, causing increased calcium uptake. • Calcium causes release of vesicles containing epinephrine.
Actions of Epinephrine • Bind to alpha-adrenergic and beta-adrenergic receptors. • Typical responses (“fight or flight”): - iris dilatation - increased heart rate - bronchodilatation - intestinal relaxation - glycogenolysis - lypolysis
hypothalamus CRF (-) pituitary ACTH cortisol adrenal gland Regulation of Cortisol Release • Cortisol release is primarily under neuroendocrine control.
gMSH aMSH clip bLPH bEndorphin } ACTH Some Additional Information: • CRF acts through a Gs-protein coupled receptor, increasing cAMP levels in pituitary corticotroph cells. • Recall that ACTH is produced by post-translational modification of proopiomelanocortin:
Action of ACTH on Cortisol Production • ACTH binds to the ACTH receptor (Gs-coupled), resulting in increased cyclic AMP and activation of PKA pathway. • This results in: - increased conversion of cholesterol esters to free cholesterol - increased expression of steroidogenic acute regulatory protein (cholesterol transfer) - increased expression of P450 side chain cleavage - increased production of IGF-II (stimulation of cell growth)
ACTH AC Gs growth ATP cyclic AMP cholesterol ester P450scc free cholesterol Action of ACTH on Cortisol Production PKA IGF-II pregnenolone cortisol
Daily Pattern of Cortisol Release • Changes in cortisol levels occur about 30 minutes after corresponding changes in ACTH. • Cortisol usually increases a few hours after sleep, then declines (it has a diurnal rhythm). • Also an increase shortly after wakening in the morning, and sporadically throughout the day. • Peaks shortly after we rise in morning. • Lowest shortly before and shortly after sleep begins. • Circadian rhythm may reflect actions required for the stress of simply living.
Transport of Cortisol • Recall that the majority of cortisol is bound to cortisol binding globulin (also called transcortin). Only 5% of circulating cortisol is in free form. • Also recall that cortisol bound to CBG is not biologically available. • CBG is produced by the liver. • Production of CBG is increased by estradiol.
Metabolism of Cortisol • Cortisol has a half-life of about 90 minutes. • Cortisol is metabolized in the liver, where it is conjugated to a glucuronic acid. - conjugation increases solubility in water - conjugated hormone is excreted via the kidneys
Functions of Cortisol • Cortisol is the primary glucocorticoid in humans. • Cortisol is essential for life. • Roles of cortisol: - carbohydrate metabolism - permissive effects on body functions and development (epinephrine release, lipid metabolism) - mineralocorticoid activity at the kidney (minor) - anti-inflammatory compound
Control of Cortisol Secretion: Feedback Loops • External stimuli • Hypothalamic • Anterior Pituitary • Adrenal cortex • Tissues Figure 23-3: The control pathway for cortisol
Role in Carbohydrate Metabolism • Cortisol has effects on nutrient metabolism: - decreases uptake of circulating glucose by muscle and adipose tissue - proteolysis of muscle protein for energy - increases lipolysis in adipose tissue for energy - at the liver, get gluconeogenesis from free fatty acids and amino acids produced by actions in muscle and adipose tissue (increases PEPCK activity) Overall, increases plasma glucose levels.
Role in Carbohydrate Metabolism • Cortisol release is inhibited by high blood glucose.
Permissive Actions of Cortisol • Cortisol is required for: - synthesis of epinephrine (adrenal medulla) - normal vasoconstriction (absence leads to decreased blood pressure) - normal glomerular filtration rate at kidney (related to blood pressure)
Effects of Elevated Cortisol on Bone • Recall that high glucocorticoid levels cause decreased bone mass. This is due to: • antagonizing the effects of vitamin D on calcium uptake • inhibiting collagen synthesis • synergizing with PTH to break down bone
Mineralocorticoid Activity of Cortisol • Under normal conditions of blood pressure and sodium levels, cortisol has some mineralocorticoid activity (increasing sodium and water reabsorption at the kidney). • Cortisol has low affinity for the mineralocorticoid receptor. • However, much more cortisol than aldosterone is secreted.
Cortisol as an Anti-Inflammatory Agent • The body responds to bacteria or tissue damage with an inflammatory response: - increased production of chemicals such as interleukins - these cause increased vasodilation and blood flow to the area - increased blood flow brings in phagocytes, mast cells, and lymphocytes - these cells trigger lysosomal reactions, histamine release, and collagenase production • Result: destruction of bacteria; healing and remodeling of tissue.
Cortisol as an Anti-Inflammatory Agent • The painful effects of healing/irritation can be treated with cortisol. • Cortisol inhibits inflammatory and immune responses: - decreased permeability of capillaries (decreasing entrance of cells to inflammed areas) - stabilization of lysosomal membranes (decreased release of lysozomes) - decreased phagocytosis by white blood cells - suppression of T lymphocytes (immune cells) - decreased synthesis of interleukins - inhibits synthesis of collagenase • Results in slower, but less painful healing.
Cortisol and Chronic Stress • Prolonged exposure to high cortisol levels can lead to break down of muscle, excessive epinephrine release, hyperglycemia, weakening of bone, destruction of the immune system, inhibition of reproductive function, and other complications. • What might be the evolutionary significance of this?
Permissive Effects of Cortisol on Development • Cortisol is required for normal development: - permissive role in final maturation of many organs - required for synthesis of digestive enzymes, surfactant - required for skeletal growth in children
AP1 cortisol AP1 site Mechanisms of Cortisol Action • The actions of cortisol are mediated through the glucocorticoid receptor. • Intracellular receptor in steroid receptor superfamily. • Stimulates transcription of target genes by interaction of bound receptor with GRE in 5’ flanking region. • Inhibits transcription of some genes by interaction of receptor with AP1 (jun/fos dimer), decreasing AP1-mediated gene expression. transcription GR
Hormone Effects on Gene Activity Cortisol
Cushing’s Syndrome • Hypercortisolism • Can be caused by pituitary or adrenal tumors • Symptoms include central obesity but thin limbs; rounded face; weak bones; weak muscles; high blood pressure; high blood glucose; fragile skin; mood swings…
Functions of Aldosterone • Aldosterone plays a major role in mineral and water balance: -increases sodium reabsorption in distal tubules of the kidney -as sodium is actively reabsorbed, also get passive absorption of water by osmosis -also get excretion of potassium (active and passive) - result: increased retention of sodium and of water • Aldosterone also increases sodium reabsorption in sweat glands.
Mechanism of Aldosterone Action • Aldosterone acts through the intracellular mineralocorticoid receptor. • Binding of hormone to the receptor results in expression of gene products that influence the rate of Na+ transport from urine back into the kidney. • Na+ and H2O reabsorption: If H2O reabsorption is impaired, and [Na+] increases, the increased osmotic pressure will activate ADH increase renal H2O reabsorption increase H2O intake by stimulating thirst.
These target genes result in: - increased availability of ATP to drive active transport - increased synthesis of Na+ transporters - increased leakiness of the membrane to Na+, so that Na+ is reabsorbed by diffusion
Influence of Aldosterone on Na+ and H2O Reabsorption and K+ Excretion Na+ Na+ H+ Aldosterone H2O H2O K+ K+ Na+ Na+ K+ K+ epithelial cell distal tubule
Binding of Cortisol to the Mineralocorticoid Receptor • In the laboratory, cortisol can bind very effectively to the mineralocorticoid receptor, resulting in activation. • However, in most tissues that express the mineralocorticoid receptor, most of the cortisol is locally converted to cortisone by 11-beta hydroxysteroid dehydrogenase. • Cortisone does not bind to the mineralocorticoid receptor very well. • Deficiency in 11-beta hydroxysteroid dehydrogenase leads to high blood pressure, due to increased mineralocorticoid activity of cortisol (genetic defect, licorice).
Role of 11-beta Hydroxysteroid Dehydrogenase in Cortisol Metabolism cortisol mineralocorticoid receptor 11-beta HSD increased retention of sodium and water from kidney cortisone
Regulation of Aldosterone Production • The main stimulator of aldosterone production is angiotensin II, not ACTH. • ACTH does have a trophic (stimulatory) effect on the zona glomerulosa, preventing atrophy.
The Renin-Angiotensin System • The juxtaglomerular cells of the kidney release renin in response to decreased blood pressure, decreased sodium levels, or sympathetic stimulation.
The Renin-Angiotensin System • Renin converts angiotensinogen (from the liver) into angiotensin I • Angiotensin I is converted to angiotensin II in a number of places in the body (ie, lungs) • Angiotensin II acts on adrenal cells to stimulate aldosterone release, and is itself a vasoconstrictor (increases blood pressure)
(-) (-) The Renin-Angiotensin System decreased Na+ (macula densa) angiotensinogen (liver) juxtaglomerular cells renin decreased blood pressure angiotensin I kidney tubules Na+ angiotensin II H2O adrenal aldosterone
Transport and Metabolism of Aldosterone • There is no specific aldosterone carrier protein • As a result, most aldosterone is biologically available, and only low levels of aldosterone release are required each day • The circulating half life of aldosterone is very short. • Aldosterone is metabolized in the liver, conjugated with glucoronide and excreted in the urine
Role of Atrial Natriuretic Factor (ANF) • ANF is produced by atria of the heart, and production is increased by increased blood pressure. • ANF inhibits aldosterone production (to inhibit resorption of water) (blocks actions of angiotensin II). • ANF also has these effects: - inhibits renin release (blocks production of angiotensin II) - decreases AVP release from posterior pituitary - causes dilation of blood vessels to decrease bp - acts directly on the kidney to increase loss of water and sodium - increased glomerular filtration rate - decreased reabsorption of sodium Net result: decreased water volume, decreased bp.