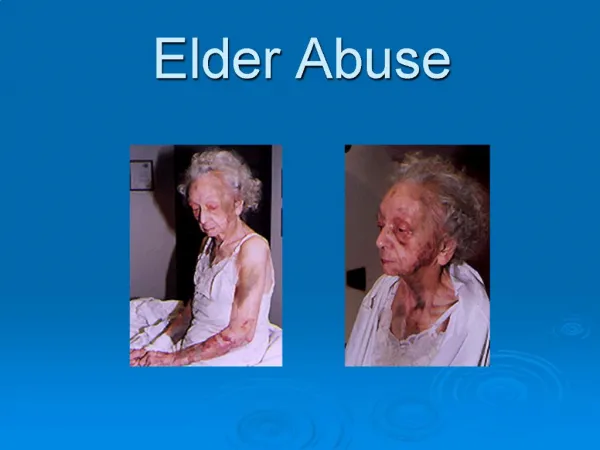
Advancements in Adult Safeguarding: The Law Commission's Action on Elder Abuse
This report analyzes the recent developments in adult safeguarding practices in response to elder abuse. It outlines new statutory duties on social services and government, establishing clearer definitions for at-risk individuals and legal frameworks for safeguarding boards. Emphasizing empowerment, protection, and prevention, the report details operational principles for local services, ensuring adequate responses to abuse. Key recommendations include enhanced cooperation across agencies, serious case reviews, and the importance of transparency and accountability in safeguarding arrangements within care settings.


Advancements in Adult Safeguarding: The Law Commission's Action on Elder Abuse
E N D
Presentation Transcript
Key points from the Law Commission: • a duty on social services to investigate or cause an investigation • into adult protection cases; and a duty on Government to • prescribe the process for such investigations; • a new definition of people at risk of abuse and of harm in order • to ensure those in need receive adequate protection; • a statutory basis for adult safeguarding boards which should as • a minimum comprise local social services, police and health; • the legal requirement to establish serious case reviews; and an • enhanced duty to cooperate between relevant organisations.
Government response: • Safeguarding Boards will be made statutory. • A statement of principles for use by Local Authority Social • Services and housing, health, the police and other agencies for • both developing and assessing the effectiveness of their local • safeguarding arrangements. • Principles: Empowerment, Protection, Prevention, • Proportionality, Partnership, and Accountability • The outcomes for adult safeguarding, for both individuals and • agencies
Empowerment: the presumption of person-led decisions and informed consent Agency objective: We give individuals relevant information about recognising abuse and the choices available to them to ensure their safety. We give them clear information about how to report abuse and crime and any necessary support in doing so. We consult them before we take any action. Where someone lacks capacity to make a decision, we always act in his or her best interests.
Protection Support and representation for those in greatest need Agency objective: Our local complaints, reporting arrangements for abuse and suspected criminal offences and risk assessments work effectively. Our governance arrangements are open and transparent and communicated to our citizens.
Prevention It is better to take action before harm occurs Agency objective: We can effectively identify and appropriately respond to signs of abuse and suspected criminal offences. We make staff aware, through provision of appropriate training and guidance, of how to recognise signs and take any appropriate action to prevent abuse occurring. In all our work, we consider how to make communities safer.
Proportionality Proportionate and least intrusive response appropriate to the risk presented. Agency objective: We discuss with the individual and where appropriate with partner agencies the proportionality of possible responses to the risk of significant harm before we take a decision. Our arrangements support the use of professional judgement and the management of risk.
Partnership Local solutions through services working with their communities. Communities have a part to play in preventing, detecting and reporting neglect and abuse Agency objective: We have effective local information-sharing and multi-agency partnership arrangements in place and staff understand these. We foster a “one” team approach that places the welfare of individuals above organisational boundaries.
Accountability Accountability and transparency in delivering safeguarding Agency objective: The roles of all agencies are clear, together with the lines of accountability. Staff understand what is expected of them and others. Agencies recognise their responsibilities to each other, act upon them and accept collective responsibility for safeguarding arrangements.
Principles in context – investigating crimes in care home settings
All investigations within a care home should be designated critical incidents and be subject to a community impact assessment. KEY POINTS: When investigating crimes within a residential care home setting, consider whether it is feasible and appropriate to use officers dressed in casual wear in order to avoid further anxiety or distress to other residents. Agree with the care home owner/manager what information can be shared with relatives, residents and staff that provides factual information about what has occurred and what is happening. Ensure that investigating officers are aware of both the potential communication needs of witnesses and what sources of support are available e.g. local advocacy providers, Independent Mental Capacity Advocates (IMCA) etc.
KEY POINTS: Investigating officers should be trained in the Mental Capacity Act (2005) and be aware that capacity is both time and decision specific. Recognising that the care home environment is the resident’s family home, and that domestic abuse perpetrators are often serial abusers, will ensure that DV strategies can be considered. Neither the police nor any member of the safeguarding team can prevent an employer from undertaking a disciplinary investigation, even where a criminal investigation has begun. Nor can anyone instruct an employer to suspend, or not suspend, an employee.
KEY POINTS: If the investigation is complex and is likely to continue for a significant period of time in excess of four weeks, it is probable that the employer will have to proceed with the disciplinary process. In such circumstances it is important that the police and employer consider carefully how to do this with least impact upon the criminal investigation. It is helpful if the senior investigating officer could provide timely updates of the criminal investigation to the care home manager and owner in terms of both the progress of the investigation and the likely timescales for completion Imposing a temporary ban on all admissions to a home, pending the outcome of the investigation, should only occur after a full risk assessment has identified that it is the only way in which such protection can be achieved successfully i.e. it has to be a proportionate and appropriate response to the type and circumstances of the allegations.
KEY POINTS: ANY OTHER SUGGESTIONS? garyfitzgerald@elderabuse.org.uk
Interview in the January 2011 Guardian: Care providers will be asking themselves, what can I do to cut corners? The sector is ready to slash costs as a result of public sector cuts. It is against this background that the Commission is signalling that it will take an increasingly tough line to ensure that essential standards are met – even when budgets are cut. The Care Quality Commission To counter the threat CQC will use an organisation that does a lot of work for the security services to scan what’s out there – either in newspapers or on the net – and identify risk. BBC December 2010 The CQC claim that 93 care homes and agencies had been shut in the past year due to poor ratings was not true.
Residents moved around in public scantily clad. The Burstow Care Home, Sutton Very personal care, such as removing dentures, undertaken in public. A resident was sat on a commode, in full view of other residents Call bells were not accessible Residents had to manage their own allergies Residents had to wipe their soiled hands on bedclothes or clothing Residents who needed help to eat and drink were left unaided Food and fluid charts not completed, or not accurately completed. Food intake record falsified in front of inspector
Paget University Hospital, Great Yarmouth Inspected on 2 April 2011 Given 28 days to produce an action plan Re-visited five months later – still failing. Given another month to improve – or serious action will be taken There was no Adult Safeguarding referral. There was no 'blanket ban' on admissions. The requirements of the Mental Capacity Act 2005 (MCA) were not applied. There was no immediate protection plan
Not Compliant Whiston Hospital (St Helens and Knowsley Teaching Hospitals NHS Trust) When we looked through records for people admitted from a care home we were unable to locate the transfer information from the care home. Staff confirmed that they usually received this but the information in them was not always easily transferred to the hospital's own records. Red trays and jugs are used to identify people who may need extra support with food and drink. On another ward only two red trays were used despite staff reporting and the CQC team observing that almost half the people needed some form of assistance.
Compliant Northwick Park Hospital (North West London Hospitals NHS Trust) One elderly patient on Evelyn Ward, who was suffering from dementia, went without food and oral fluids from midnight on three consecutive days until his operation was cancelled each day. On the day of our visit he was provided with a cup of tea when the nurse became aware the operation had been cancelled at three o’clock. The patient had been nil by mouth for fifteen hours until then although he had received intravenous fluids. This put the patient at risk of inadequate nutrition as well as unnecessary discomfort.
Compliant Royal Devon and Exeter NHS FoundationTrust at Wonford, ‘We asked if patients had DNAR orders. Staff confirmed that some patients did. We asked them to give an example of someone on the ward that had a DNAR order and how and when this decision was reached. They gave the example of a patient with a DNAR order whose decision for this was made due to being 'elderly and with co-morbidities that make resuscitation less appropriate'. We asked for more detail about being elderly and co-morbidities. We were told that the DNAR order had been made on admission. A doctor said that the main factor would be the patient's medical status. The doctor was not aware if the patient or their advocate/ relatives had been involved in the decision making for the DNAR, or how the views of a patient with dementia are sought beyond taking to the nursing staff to find out what information they have. The doctor said that if the team are aware of advance directives that this is taking into account, however none of the care records we looked at had this part completed.’
Not Compliant Alexandra Hospital (Worcestershire Acute Hospitals NHS Trust). One person was assessed as being ‘malnourished ‘on admission and there were no details of their weight at that time. They were not reassessed until 16 days later. The records for another person showed they were seen by a dietitian on admission and the following day and on each occasion a request had been made to weigh the person. Notes 17 days later referred to the fact that the person had not been weighed since admission. We looked at records of fluid intake and output for some people and saw that some people had received no fluids for long periods of time. In some cases this exceeded 10 hours.
Care Quality Commission • The Care Quality Commission (CQC) is the independent regulator of all health and adult social care in England. • Whether care services are provided by the NHS, local authorities or voluntary organisations, CQC say that they make sure that people get better care. They say they do this by: • encouraging improvement across health and adult social care • putting people first and standing up for their rights • acting quickly to remedy bad practice • gathering and using knowledge and expertise, and working with others.
Elder Abuse Helpline 080 8808 8141 Admin telephone: 020 8835 9280 WEBSITE: WWW.ELDERABUSE.ORG.UK garyfitzgerald@elderabuse.org.uk