Download
1 / 98
1.05k likes | 1.95k Vues
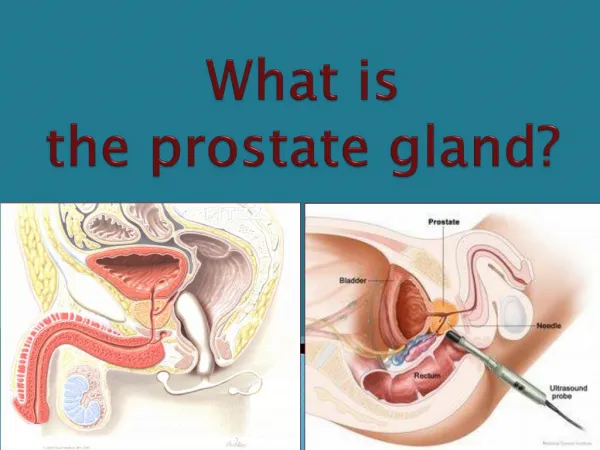
Neoplasms of the Prostate Gland. Prostate gland. Made of two lobes, enclosed by an outer layer of tissue Located in front of the rectum and just below the bladder, where urine is stored Blood supply: internal iliac artery -inferior vesical artery -middle rectal artery

E N D
Prostate gland • Made of two lobes, enclosed by an outer layer of tissue • Located in front of the rectum and just below the bladder, where urine is stored • Blood supply: internal iliac artery -inferior vesical artery -middle rectal artery • Venous drainage: dorsal venous complex IJV • Innervation: pelvic plexus
Prostate Gland • Peripheral zone 70% -Prostate cancer • Central zone 25% • Transition zone 5% -BPH
Benign Prostatic Hyperplasia • Most common benign tumor in men • Incidence is age related • 20% in men aged 41-50 • 50% in men aged 51-60 • >90% in men aged >80 • Risk Factors: -genetic : autosomal dominant -racial differences
Benign Prostatic Hyperplasia Pathology: • BPH develops in the transition zone • Results from increase in cell number • Microscopic: nodular growth pattern, varying amounts of stroma and epithelium • Compress the outer zones of the prostate (surgical capsule) • bladder outlet resistance due to mechanical obstruction
Benign Prostatic Hyperplasia Clinical Findings: Symptoms: • Obstructive -hesitancy -decreased force and caliber of stream -sensation of incomplete bladder emptying -double voiding • Irritative -urgency -frequency -nocturia
Benign Prostatic Hyperplasia Signs • P.E., DRE and focused neurologic exam • Size and consistency • Smooth, firm, elastic enlargement -PSA -TRUS -biopsy
Benign Prostatic Hyperplasia Laboratory findings • Urinalysis- to exclude infection or hematuria • Serum creatinine measurement- to assess renal function • Serum PSA- optional , increased ability to detect CaP • DRE- general idea of the size and condition of the gland Imaging • Upper tract imaging ( Intravenous pyelogram or renal ultrasound)- recommended only in presence of concomitant urinary tract disease
Benign Prostatic Hyperplasia • Prostate Biopsy • Cytoscopy- to determine the size of the gland and identify the location and degree of the obstruction. • Additional Tests: cystometrograms and urodynamin profiles.
Microscopic examination of different types of prostate tissues (stained with immunohistochemical techniques): A. Normal (non-neoplastic) prostatic tissue (NNT). B. Benign prostatic hyperplasia. C. High-grade prostatic intraepithelial neoplasia (PIN). D. Prostatic adenocarcinoma (PCA).
Benign Prostatic Hyperplasia • Differential Diagnosis -urethral stricture hx of urethral instrumentation, - bladder neck contracture urethritis, trauma -bladder stone: hematuria and pain -Prostate Cancer -UTI: do urinalysis and culture -neurogenic bladder disorders: history of neurologic disease, stroke, DM
Benign Prostatic Hyperplasia • Treatment -mild symptoms: watchful waiting -surgical indications: recurrent UTI refractory urinary retention recurrent gross hematuria bladder stones renal insuficiency large bladder diverticula
Benign Prostatic Hyperplasia • Medical Therapy 1. Alpha blockers -prostate and bladder contains alpha-1-adrenoreceptors - improvement in signs and symptoms - Phenoxybenzamine, prazosin 2. Alpha reductase inhibitors -Finasteride -blocks conversion of testosterone to dihydrotestosterone -reduce size of gland and improvement of symptoms
Benign Prostatic Hyperplasia • Medical Therapy 3. Combination Therapy - 5-alpha reductase inhibitor + alpha blocker 4. Phytotherapy - use of plants or plant extracts -popular in Europe and US
Conventional Surgical Therapy • Transurethral Resection of the Prostate (TURP) • Transurethral Incision of the Prostate • Open simple prostatectomy
Transurethral resection of the Prostate • Superior symptom score and flow rate improvement than minimally invasive therapy • Longer length of confinement • Risks: • Retrograde ejaculation • Impotence • Incontinence
TURP An enlarged prostate can cause urinary problems due to its location around the male urethra (A). In TURP, the physician uses a cystoscope to gain access to the prostate through the urethra (B). The prostate material that has been restricting urine flow is cut off in pieces, which are washed into the bladder with water from the scope (B). (Illustration by GGS Inc.)
Transurethral Resection of the Prostate • Complications : • Bleeding • Urethral stricutre or bladder neck contracture • Perforation of the prostate capsule with extravasation • TUR syndrome hypervolemic, hyponatremic state due to absorption of the hypotonic irrigating solution
TUR syndrome • Nausea • Vomiting • Confusion • Hypertension • Bradycardia • Visual disturbances • *risk increases with resection time >90 minutes • Tx : diuresis • Hypertonic saline administaration
Transurethral incision of the prostate • Moderate to severe symptoms • Small prostate • * posterior commissure hyperplasia: elevated bladder neck • More rapid • Less morbid • Lower rate of retrograde ejaculation(25%)
Transurethral Incision of the Prostate • Technique • Collin’s knife 5 and 7 o’clock positions • Incision distal to the ureteral orifices and are extended outward to the verumontanum
Open Simple prostatectomy • Prostate is too large to be removed endoscopically • Open enucleation • “large” vary depending on the surgeon’s experience with TURP • >100 grams • Concomitant bladder diverticulum • Bladder stone • Dorsal lithotomy positioning is not possible • Can be Simple suprapubic prostatectomy or Simple retropubic prostatectomy
Open Simple Prostatectomy • Simple suprapubic prostatectomy • Performed transvesically, operation of choice if with concomitant bladder pathology • Semicirucular incision in the bladder mucosa., distal to the trigone • Hemostasis attained with suture ligature • Urethral and suprapubic catheter – before closure
Open Simple prostatectomy • Simple retropubic prostatectomy • Bladder not entered • Transverse incision made in the surgical capsule of the prostate • Urethral catheter - end of the procedure
Minimally Invasive Therapy 1. Laser therapy 2. Transurethral electrovaporization of the prostate 3. Hyperthermia 4. Transurethral needle ablation of the prostate 5. High-intensity focused ultrasound 6. Intraurethral stents
1. Laser Therapy • Two main energy sources – Nd:YAG and holium:YAG • Techniques: a. Coagulation necrosis technique b. Visual contact ablative technique c. Intersitial laser therapy
Coagulation Necrosis Techniques • Transurethral laser-induced prostatectomy (TULIP) with TRUS guidance • Do not create an immediate visual defect in the prostatic urethra • Tissue sloughed : several weeks – 3 months following the procedure
Visual Contact Ablative techniques • More time consuming • Fiber placed in direct contact with the prostate tissue • Immediate defect is obtained
Interstitial laser therapy • Fibers directly into the prostate, cystoscopic control • Laser is fired submucosalcoagulative necrosis • Urethral mucosa is spared prostate tissue is reabsorbed by the body ↓ irritative voiding symptoms
ADVANTAGES • Minimal blood loss • Rare instaces of TUR syndrome • Ability to treat patients receiving anticoagulation therapy • Ability to be done as an outpatient procedure
DISADVANTAGE • Lack of availability of tissue for pathologic examination • Longer postoperative catheterization time • More irritative voiding complains • High cost of laser fibers and generators
2. Transurethral Electrovaporization of the Prostate • Use standard resectoscope – grooved rollerball • High current densities cause heat vaporization of tissue cavity in the prostatic urethra • Takes longer than a standard TURP
Transurethral Microwave Thermotherapy 3. Hyperthermia TUMT • Microwave hyperthermia – delivered with a transurethral catheter • Deliver microwave energy to the prostate,high temperatures kill prostate cells • Sensors on the catheter and on a tube in the rectum enable monitoring of the temperatures throughout the procedure, and a cooling system circulates water within the catheter to protect the urethra.
4. Transurethral needle ablation of the Prostate (TUNA) • Specially designed urethral catheter where radio frequency needles are deployed coagulative necrosis • Not adequate in treating bladder neck and median lobe enlargement
5. High-intensity focused ultrasound • Thermal ablation • Dual-function ultrasound probe (rectum) • Transrectal imaging of the prostate • Delivers short bursts high-intensity focused ultrasound energy • Coagulative necrosis • Bladder neck and median lobe enlargement are not adequately treated
6. Intraurethral Stents • Endoscopically placed in the prostatic fossa • Keep the prostatic urethra patent • For patients with limited life expectancy, not appropriate candidates for surgery or anesthesia
Carcinoma of the PROSTATE • Most common cancer detected in American men • Second leading cause of cancer death in men, mortality rates have been declining since the mid-1990’s • Major health-care concern unless more effective forms of prevention and treatment are identified • Prevalence increases most rapidly with age
Carcinoma of the PROSTATE • CaP continues to increase with advancing age • Lifetime risk of a 50-year-old man for: • Latent: 40% • Clinically apparent: 9.5% • Death from - : 2.9% • Many prostate cancers are indolent and inconsequential to the patient while others are virulent, and if detected too late or left untreated, they result in a patient’s death
Carcinoma of the PROSTATE • African American > white • Diet • Total fat, animal fat, red meat, Vitamin D and Calcium - ↑ • Fish, lycopene selenium, omega03 FA, Vitamin E - ↓ • Risk factors: • Increasing age • < 40 : 1 in 10,000 • 40-59: 1 in 103 • 60-79: 1 in 8 • (+) Family Hx • Age of disease onset in the family member affects patient’s relative risk • 70 y/o : 4x • 60 y/o: 5x • 50 y/o: 7x • BRCA1 and BRCA2 genes have two to five times higher risk of prostate cancer.
Molecular Genetics and Pathobiology • Molecular profiling of human tissues • Diagnostic, prognostic and therapeutic markers have been discovered • Chromosomal rearrangements or copy number abnormalities described in Prostate CA • 8p, 10q, 11q, 13q, 16q, 17q, and 18q • Specific loss at 8p23.2 and/or gain at 11q13.1 : predictive of prostate CA progression
Molecular Genetics and Pathobiology • Inflammation may be related to prostate CA development • Candidate- inherited susceptibility genes for prostate CA including familial cancer: • RNASEL: encoding an interferon inducible ribonuclease • MSR1: encoding subunits of the macrophage scavangerreceptro
Pathology • ~95% : Adenocarcinoma • ~5% : nonadenocarcinoma • 90% : transitional cell carnicomas • 10% neuroendocrine (“small cell”) carcnomas or sarcoma • Histology: heterogenous, arising from stromal epithelial, or ectopic cells.
Adenocarcinoma • Cytologic characteristics of CaP: • Hyperchromatic. Enlarged nuclei with prominent nucleoli • Cytoplasm, often abundant • Slightly blue tinged or basophilic • Basal cell layer is absent • high molecular weight keratin immunohistochemical staining, preferentially stains basal cells • Markers: AMACR or EPCA • Useufl to identify those with the disease, but who have equivocal or negative biopsies on standard tissue staining