Download
1 / 20
240 likes | 662 Vues
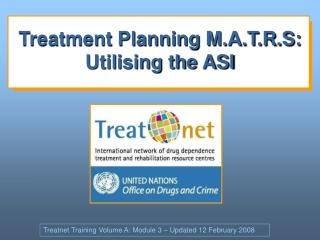
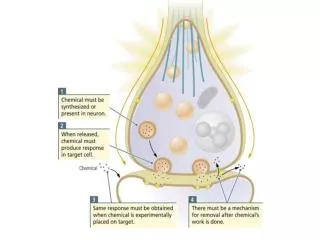
Muscarinic Receptors: Rationale for OAB Treatment. Dr. Michael Ruggieri, Sr. Department of Urology Temple University, Philadelphia, PA . Bladder: Anatomy and Function. CNS inhibitory/stimulatory. M 2 ; M 3 Muscarinic Receptors. Sympathetic-Hypogastric Nerve. ParasympatheticPelvic Nerve.

E N D
Muscarinic Receptors: Rationale for OAB Treatment Dr. Michael Ruggieri, Sr. Department of Urology Temple University, Philadelphia, PA
Bladder: Anatomy and Function CNS inhibitory/stimulatory M2; M3 Muscarinic Receptors Sympathetic-Hypogastric Nerve ParasympatheticPelvic Nerve Bladder Detrusor Smooth muscle SomaticPundal Nerve Internal Sphincter Smooth Muscle Extramural Skeletal Muscle Wein, Exp. Opin. Invest. Drugs 10(1): 65-83, 2001
Muscarinic Receptors Muscarinic receptors are identified primarily on the basis of the effect and relative potency of selective agonistsand antagonists Five subtypes have been identified. In peripheral tissues the role of three are well established: • M1 - Autonomic ganglia of secretory glands, presynaptically in bladder • M2 - Heart and bladder (smooth muscle) and presynaptically in bladder • M3 - Smooth muscle and secretory glands All 3 also found in the CNS
Gβγ proteins (M2) Gα proteins (M1,3,5) RGS-4 PI3 Kinase PLA2 & PLD PIP3 PLD PKG-I PC-PLC RhoA Arachidonic Acid Atypical PKC Ca++ Channels ROCK DAG cAMP PKC PKA and PKG Non-selective Cation channels Ca++ CPI-17 MYPT1 Ca++ ? Ca++ Dependent K channel MLC Phosphatase Inhibition Activation Relaxation Both Necessary For activation Normal Contractions Receptor Activation Gα proteins PI-PLC IP3 IP3 Receptor Calmodulin Activation SR calcium Release MLC Kinase MLC Muscle Contraction
Gβγ proteins (M2) Gα proteins (M1,3,5) PiPLC inhibitor ET-18-OCH31 PI3 Kinase RGS-4 PLA2 & PLD PIP3 PKG-I PI-PLC PC-PLC Arachidonic Acid Atypical PKC Ca++ Channels IP3 cAMP PKA and PKG IP3 Receptor Non-selective Cation channels Ca++ MYPT1 SR calcium Release Calmodulin Activation Ca++ ? Ca++ Dependent K channel MLC Kinase Inhibition Activation Relaxation Both Necessary For activation Normal Contractions (PI-PLC Inhibition) Receptor Activation Gα proteins PLD RhoA ROCK DAG PKC CPI-17 MLC MLC Phosphatase Muscle Contraction Decreased Agonist Potency 1. Braverman, A.S., Tibb, A.S. and Ruggieri, M.R. J Pharmacol Exp Ther, 316: 869-874, 2006.
Y-276321 Gβγ proteins (M2) Gα proteins (M1,3,5) PI3 Kinase RGS-4 PLA2 & PLD PIP3 PLD PKG-I PC-PLC RhoA Arachidonic Acid Atypical PKC Ca++ Channels ROCK DAG cAMP PKC PKA and PKG Non-selective Cation channels Ca++ CPI-17 MYPT1 Ca++ ? Ca++ Dependent K channel MLC Phosphatase Inhibition Activation Relaxation Both Necessary For activation Normal Contractions (ROCK Inhibition) Receptor Activation Gα proteins PI-PLC IP3 IP3 Receptor Calmodulin Activation SR calcium Release MLC Kinase MLC Muscle Contraction Decreased Agonist Potency 1. Braverman, A.S., Tibb, A.S. and Ruggieri, M.R. J Pharmacol Exp Ther, 316: 869-874, 2006.
PiPLC inhibitor ET-18-OCH31 U-731222 Gα proteins Inhibition Activation Both Necessary For activation Denervated1 or M3 Desensitized By Repeated CRC2 (PI-PLC Inhibition) Receptor Activation Gβγ proteins (M2) Gα proteins (M1,3,5) PI3 Kinase RGS-4 PLA2 & PLD PIP3 PLD PKG-I PI-PLC PC-PLC RhoA Arachidonic Acid Atypical PKC Ca++ Channels ROCK IP3 DAG cAMP PKC PKA and PKG IP3 Receptor Non-selective Cation channels Ca++ CPI-17 MYPT1 Calmodulin Activation Ca++ SR calcium Release ? Ca++ Dependent K channel MLC Kinase MLC MLC Phosphatase Muscle Contraction Relaxation No Change in Agonist Potency 1. Braverman, AS, Doumanian, LR and Ruggieri, MR J Pharmacol Exp Ther, 316: 875-880, 2006. 2. Schneider T, Hein P, Michel MC. J Pharmacol Exp Ther, 308(1):47-53,2004.
Y-276321 Gβγ proteins (M2) Gα proteins (M1,3,5) PI3 Kinase RGS-4 PLA2 & PLD PIP3 PLD PKG-I PC-PLC RhoA Arachidonic Acid Atypical PKC Ca++ Channels ROCK DAG cAMP PKC PKA and PKG Non-selective Cation channels Ca++ CPI-17 MYPT1 Ca++ ? Ca++ Dependent K channel MLC Phosphatase Inhibition Activation Relaxation Both Necessary For activation Denervated1 or M3 Desensitized By Repeated CRC2 (ROCK Inhibition) Receptor Activation Gα proteins PI-PLC IP3 IP3 Receptor Calmodulin Activation SR calcium Release MLC Kinase MLC Muscle Contraction Decreased Agonist Potency 1. Braverman, AS, Doumanian, LR and Ruggieri, MR J Pharmacol Exp Ther, 316: 875-880, 2006. 2. Fleichman M, Schneider T, Fetscher C, Michel MC. J Pharmacol Exp Ther, 308(1):54-8, 2004.
M2 / M3 in the Bladder Wall Section of Bladder Wall Umbrella Cell Bladder lumen Endothelium Lamina Propria M2 Muscarinic Receptor M3 Muscarinic Receptor Smooth Muscle
Increased bladder capacity by antimuscarinics depends on C-fiber afferents • Yokoyama, O. et al. J Urol, 174, 2032-2036, 2005. • Suzuki, M et al. Eur J Pharmacol, 512, 61-66, 2005
Chronic syndrome with debilitating symptoms defined as: Urgency, with or without urgency incontinence, often accompanied by frequency and nocturia Overactive Bladder (OAB)
Antimuscarinic Agents Oxybutynin Tolterodine H3C CH3 COOH OH H CH OH CH3 N C2H5 O • HO CH H3C N C CH2 C C CH2 C O • HCl COOH CH3 C2H5 OH Trospium Chloride O N+ C OH O Solifenacin Darifenacin O N O NH2 O O N N
Muscarinic Binding Studies M3 : M2 M2 M3 Agent 1.3 Trospium3 9.2 9.3 3.2 Tolterodine1 8.0 8.5 12.6 7.8 8.9 Oxybutynin1 12.6 6.9 8.0 Solifenacin2 50.1 7.4 9.1 Darifenacin1 1. Wallis RM, Napier CM. Life Sci. 1999;64:395-401.2. Ikeda K, et al. Naunyn-Schmiedeberg’s Arch Pharmacol. 2002;366(2):97-103. 3. Napier C, et al. Proc ICS. 2002;445 (abstract).
50 40 30 20 10 0 Muscarinic Receptor Balanced Selectivity M3:M2 1.0 = “Equipotent” M3 selective M3;M2 Selectivity Relatively M3 selective Relatively equipotent (M2/M3) Trospium Tolterodine Solifenacin Oxybutynin Darifenacin 12.6 12.6 50.1 1.3 3.2 1. Wallis RM, Napier CM. Life Sci. 1999;64:395-401.2. Ikeda K, et al. Naunyn-Schmiedeberg’s Arch Pharmacol. 2002;366(2):97-103. 3. Napier C, et al. Proc ICS. 2002;445 (abstract).
Inhibitory Function of Antimuscarinics Urothelium-derived ATP ACH Release from nerves and urothelium(?) Stretch of detrusor cells Antimuscarinic agents Suburothelial afferent nerves activation (M2,M3) Increased mygenic activity (M2,M3) Intramural afferent nerves activation (M2) Afferent nerve Urgency/micturition Andersson K. Lancet Neurol 2004; 3: 46-53
Summary • Overactive Bladder is an imbalance of afferent and efferent input • Both M2 and M3 may play a role in the sensory and myogenic pathways • The role of systemic and intravesical administration of drugs requires further study
Afferent Efferent Bladder: Anatomy and Function
Sympathetic nerve terminal Parasympathetic nerve terminal ACh NE M1 M2/4 – + ACh Ca2+ NE M2 DG 3 ROC Ca channel M3 PIP IP3 Gs AC Gi Gq PLC Ca2+ + Ca2+ – Ca2+ Ca2+ + cAMP IP3 Ca2+ Ca2+ tone contraction SR Muscarinic Receptors
Urothelium Basal membrane IC Lamina propria Muscularis mucosae IC Detrusor C-fiber Ad fiber C-fiber IC = interstitial cells
Cl- Cl- N+ N+ HO HO O O O O URGENCY Urothelium ACh+ PGs+ ATP+ NO - Basal membrane IC TKs+ PACAP- VIP- Lamina propria Muscularis mucosae IC Detrusor C-fiber Ad fiber C-fiber IC = interstitial cells K-E Andersson, 2005