Download
1 / 44
1.62k likes | 4.03k Vues
Basics of enteral and parenteral nutrition. Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training. Objectives. To discuss the different feeding pathways for the surgical patients

E N D
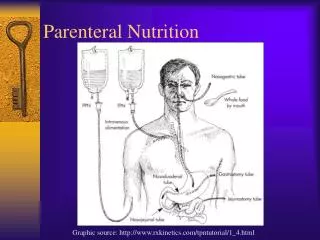
Basics of enteral and parenteral nutrition Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training
Objectives • To discuss the different feeding pathways for the surgical patients • To define and discuss key points of enteral and parenteral nutrition • To discuss the monitoring process and expected outcomes for surgical patients
Feeding Pathways Can the GIT be used? “Inability to use the GIT” Yes No “inadequate intake” Parenteral nutrition Oral Tube feed < 75% intake Short term Long term More than 3-4 weeks Central PN Peripheral PN Yes No NGT A.S.P.E.N. Board of Directors. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients, III: nutritional assessment – adults. J Parenter Enteral Nutr 2002; 26 (1 suppl): 9SA-12SA. Gastrostomy Nasoduodenal or nasojejunal Jejunostomy
Early enteral nutrition: definition • Enteral nutrition that is initiated within 24 – 48 hours following hospitalization, trauma, or injury Zaloga GP. Crit Care Med 1999; 27: 259
Why early enteral nutrition? • The normal and designed route for nutrient intake, digestion, and absorption • Immunocompetence is a major function of the gastrointestinal tract • Non-utilization of the gastrointestinal tract even on a short term basis leads to complications in critical care or geriatric patient management • Cost-effective
Early enteral feeding: goal • To maintain intestinal mucosal integrity – Normal microvilli • Height and number – Normal intestinal barrier – Intestinal mucosal immunity
Early enteral feeding: rationale • Provide nutrients required during metabolic stress • Maintain GI integrity • Reduce morbidity compared with parenteral nutrition • Reduce cost compared with parenteral nutrition
Comparison: mortality Heyland et al. JAMA, 2001 Outcome: early enteral nutrition vs. control Treatment n/N Control n/N Study 1/11 1/9 Cerra et al 1990 2/17 1/14 Gottschlich et al, 1990 0/19 Brown et al, 1994 0/18 1/51 Moore et al, 1994 2/47 24/163 12/143 Bower et al, 1996 1/16 Kudsk et al, 1996 1/17 20/87 Ross Products, 1996 8/83 7/18 Engel et al, 1997 5/18 1/22 Mendez et al, 1997 1/21 2/16 Rodrigo et al, 1997 2/13 2/16 Weimann et al, 1998 4/13 96/197 86/193 Atkinson et al, 1998 17/89 Galban et al, 2000 28/87 Pooled Risk Ratio 0.01 0.1 1 10 100 Higher for control Higher for treatment Early enteral nutrition vs standard nutritional support on mortality
JEJUNUM STOMACH Nasojejunal tube Nasogastric tube PEJ PEG BUTTON JET-PEG PLG PLJ Witzel, Stamm, Janeway NCJ PSJ PSG PFJ PFG E: Endoscopic G: Gastrostomy J: Jejunostomy Loser C et al. ESPEN guidelines on artificial enteral nutrition – Percutaneous endoscopic gastrostomy (PEG) L: Laparoscopic NC: Needle Catheter S: Sonographic F: Fluoroscopic Enteral nutrition access
Nasogastric tube Nasoentericor jejunal tube PEG tube Access and delivery
Gastrostomy PEG placement PEG placement, St Luke’s Medical Center
Long Term (operative) Jejunostomy – Percutaneous endoscopic jejunostomy or through the PEG tube – Surgical jejunostomy Short Term Nasoenteric – Nasoduodenal – Nasojejunal Post-pyloric feeding Gauderer MW, et al. J Pediatr Surg 1980;15:872-875
Enteral Formulas – what type? • Polymeric formulas (80-90%) • Commercial (preferred) • Blenderized (If not critically ill, not severely malnourished) • Oligomeric formulas • Disease-specific formulas • Modular formulas (concentrated protein and carbohydrate preparations)
Enteral nutrition delivery Gravity Feeding Enteral Pump Delivered
Practical points: enteral nutrition • If intake is within the range of 60% to 70% start oral supplement • Choose the product or preparation that meets all the daily requirements • If oral intake is 50% or less • You may give parenteral nutrition to supplement (good for a week – expensive, but more comfortable for the patient) • Cost-effective: NGT • If tube feeding duration will exceed 2 weeks and you are looking at long term (stroke or critical care) – gastrostomy is easier to maintain with lesser complications (aspiration)
Practical points: enteral nutrition • If patient will undergo surgery and you doubt patient will be able to have adequate intake for longer term: • Place gastrostomy during the surgery • If gastric function return is in doubt for more than a week: • Gastrostomy with jejunostomy tube extension • Surgical Jejunostomy • Main goal: adequate intake
Enteral formula: commercial vs. blenderized Gallagher-Alfred. Nutrition Supp Svc 1983; Tanchoco CC, et al. Respirology 2001;6:43-50 Sullivan MM, et al. J Hosp Infect 2001;49:268-273
Standard Feed: measured vs. expected Commercial formula Natural food formula Commercial formula Natural food formula Sullivan MM et al. Nutritional analysis of blenderized diets in the Philippines (PENSA 1998)
Monitoring Gastric Residuals • Monitor according to hospital protocol (e.g., every 3-4 hours) • Volume not to exceed 50% of the amount infused Mentec H, et al. Crit Care Med 2001;29:1955-1961
Parenteral nutrition: Indications • To avoid periods of starvation within 24 to 72 hours when oral or enteral intake are insufficient to achieve adequate intake in moderate to severe malnourished patients • When unable to use the gut • Gut obstruction • Short bowel (intestinal failure) • High output enterocutaneous fistulae • Non-functional gastrointestinal tract ESPEN Guidelines on Parenteral Nutrition. Clin Nutr 2009; 28(4): 359-479.
Contraindications to PN • Gut can be used: • Ability to consume and absorb adequate nutrients orally or by enteral tube feeding • Hemodynamic instability • *Ineffective and probably harmful in non-aphagic oncological patients in whom there is no gastrointestinal reason for intestinal failure. .* Bozzetti F, Arends J, Lundholm K, et al. ESPEN Guidelines on Parenteral Nutrition: Non-surgical oncology. Clin Nutr 2009; 28(4): 448.
Types of parenteral nutrition Central Peripheral Total kcal limited by concentration and ratio to volume being administered (usually delivers between 1000 to 1500 kcal/day) The current formulations can now deliver the daily requirements of macro and micronutrients Osmolality < 700 mOsm/kg No volume restriction • Amino acids ( > 5%) • Dextrose ( > 20%) • Lipids • Includes vitamins, minerals, and trace elements • Carrier of pharmaconutrients like glutamine or omega-3- fatty acids • Osmolality ( > 700 mOsm/kg H2O) • Volume restriction
Types of parenteral nutrition • Central parenteral nutrition • Peripheral central parenteral nutrition PICC =peripherally inserted central catheter
Catheters Subclavian catheter (3 ports) PICC line catheters
Types of parenteral nutrition • Peripheral parenteral nutrition
Central venous access • Allows delivery of nutrients into the superior vena cava or right atrium • Osmolarity - traditional cut off > 860 mOsm/L • Catheter differences : • According to duration of use • Various lengths, gauges, and number of ports • Catheters treated with antibacterials • Nutrient infusion via a dedicated catheter lumen • Pittiruti M et al. ESPEN Guidelines on Parenteral Nutrition: Central Venous Catheters. Clin Nutr 2009; 28(4): 365-7.
Formulations • 1 Optimal nitrogen sparing is shown to be achieved when all components of the parenteral nutrition mix are administered simultaneously over 24 hours. • The different forms of PN packaging and delivery: • 2 Individualized • 2 Compounded • 1,2 “All in One” Braga M et al. ESPEN Guidelines on parenteral nutrition. Clin Nutr 2009; 28(4): 382. Kumpf VG et al, ASPEN Nutrition Support Practice Manual 2nd ed 2005; 97-107.
Formulation / Delivery Development phases of the PN container system Individualized delivery system Compounding / clean rooms Break seal • cheaper • stable • none to minimum contamination “All in one” placed in multi-chambered bags
Safety issues • In-lineFilters: • Fat emulsions • Three in one solutions • Micro-precipitates • Protocols: • Compounding • Incorporation – additives • Delivery (access, rates of infusion, infusion pumps) Three in one bags: longer storage and less contamination
EN/PN monitoring parameters Assessment • Nutrient balance (calorie & protein intake) • Body weight • Nitrogen balance • Plasma protein (albumin, pre-albumin) Metabolic • Glucose • Fluid and electrolyte balance • Renal and hepatic function • Triglycerides and cholesterol • Campbell SM, Bowers DF. Parenteral Nutrition. In: Handbook of Clinical Dietetics. Yale University Press, 1992 • Ch 17: parenteral nutrition. Total Nutrition Therapy ver. 2, 2003; 311-12.
Key monitoring points • Fluid balance – avoid fluid accumulation within 4-5 days post op • Calorie balance • Gastric retention for enteral nutrition • Blood tests: • BUN high – dialyze • High triglycerides – lower lipid flow • Hyperglycemia – insulin • Weight once a week Jan Wernermann, “ICU Cookbook”.Franc-Asia Workshop, Singapore, 2003
Feeding Pathways Can the GIT be used? “Inability to use the GIT” Yes No “inadequate intake” Parenteral nutrition Oral Tube feed < 75% intake Short term Long term More than 3-4 weeks Central PN Peripheral PN Yes No NGT A.S.P.E.N. Board of Directors. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients, III: nutritional assessment – adults. J Parenter Enteral Nutr 2002; 26 (1 suppl): 9SA-12SA. Gastrostomy Nasoduodenal or nasojejunal Jejunostomy
Adequate intake in surgery patients Del Rosario D, Inciong JF, Sinamban RP, Llido LO. The effect of adequate energy and protein intake on morbidity and mortality in surgical patients nutritionally assessed as high or low risk. Clinical Nutrition Service, St., Luke’s Medical Center, 2008.
Nutrition team and intake Llido et al. Nutrition team supervision improves intake of critical care patients in a private tertiary care hospital in the Philippines: report from years 2000 to 2011 (for submission)