Download
1 / 46
910 likes | 2.05k Vues
ENTERAL NUTRITION. SWAPNA CHATURVEDI DIETICIAN DEPARTMENT OF DIETETICS AIIMS. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. What is Nutritional Support

E N D
ENTERAL NUTRITION SWAPNA CHATURVEDI DIETICIAN DEPARTMENT OF DIETETICS AIIMS www.anaesthesia.co.inanaesthesia.co.in@gmail.com
What is Nutritional Support “The provision of nutrients orally, enterally, or parenterally with therapeutic intent. This includes, but is not limited to, provision of total enteral or parenteral nutrition support,and provision of therapeutic nutrients to maintain and /or restore optimal nutrition status and health.” ASPEN, 2002
Who requires nutritional support? • Patients already with malnutrition- surgery/trauma/sepsis • Patients at risk of malnutrition Reasons for malnutrition: • Cannot meet nutrient requirements • Have documented inadequate oral intake • Need a prolonged period of NPO/bowel rest
Advantages of EN • More economical, effective, simple and safe • It maintains gut mucosal physiology • Preserves gut barrier function • Promotes peristalsis • Modulates immune response • Inexpensive compared with PN
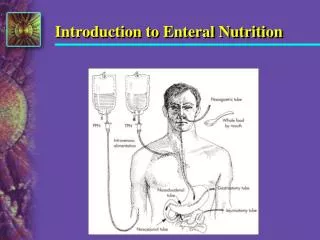
Enteral Nutrition Enteral Nutrition is delivering of nutrition to the GI tract via artificial means. Is EN Feasible? Guiding Principles: A clinical assessment of intestinal function is required to ensure safety. EN should be prescribed only if safety and a low complication rate can be ensured. A good determinant of safe tolerance of EN is a GI output of less than 600 ml/24 hr (e.g.,effluent from a ostomy, fistula).
Enteral Access Selection • Anticipated length of therapy • Degree of aspiration risk or tube displacement • Presence or absence of normal digestion • Planned surgical/endoscopic intervention • Administration and infusion schedule • Patient comfort/quality of life
EN Access Contd...
EN Access Contd...
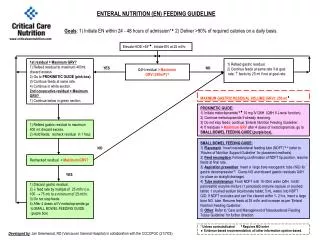
Protocol for administration of EN • Delay should be avoided. • Ideally within 48 hours of admission to stimulate guts function. • Administered as bolus feeds or by a constant feeding or intermittent feeding. Contd...
Protocol for administration of EN • Start EN –feeding with the rate of 15ml per hour of FS formula and step wise by 15ml/hour every 12 hours to reach of maximum of 60 ml/hour, provided no symptoms of intolerance. • Maintain 60ml/hr for 24 hrs, by 15ml/hr every 12 hrs. to reach a specific goal, do not exceed 100 to 120ml/hr. • Beyond this rate chances of aspiration .
Standing Instruction for Enteral Nutrition (Tube Feeding) • Physician to place feeding tube. • Check position of feeding tube: chest/ abdominal X – ray. • Do not feed until tube tip – position is documented. • Elevate head of bed > 30o during enteral feeding. Contd….
Standing Instruction for Enteral Nutrition (Tube Feeding) • Aspirate the tube 4 hourly in case of continuous feeding and prior to each feeding in case of intermittent feeding, using a 50 ml or larger syringe. – If aspirate < 150 ml, return aspirate and continue feeding. - If aspirate >150 but < 300 ml, reduce feeding rate, notify physician, consider prokinetics. - If aspirate > 300 ml, hold feeding, notify physician and assess cause. Physician may consider use of prokinetics or nasoenteral feeding or partial parenteral nutrition or reduce feeding rate by 50%. Contd….
Irrigate tube 4 hourly with 30 ml water and 12 hourly with 10 ml normal saline with a 50 ml or larger syringe. • Enteral pump can be used for continuous feeding with adjustable knob IV set. • Do not let formula hang for longer than 8 hours. • Administration set to be changed every 24 hours. • Vital signs every 2 hours. Contd...
Intake and output every 8 hours. • Weigh the patient alternate days if possible. Minimum once a week. • Irrigate tube before and after each medication. • Blood count, serum proteins, renal and liver function tests – twice a week. • Electrolytes everyday. Contd...
Assessment Obtain admission weight and usual weight as percentage of IBW • 200% IBW : Morbidly obese • 126 –199% IBW : Obese • 111 –125% IBW : Over weight • 90 –110% IBW : Adequate energy reserve • 80 –89% IBW : Lean body or mildly depleted energy stores • 70–79 % IBW : Moderate depletion of energy reserve • < 69% IBW : Severe depletion of energy reserve
Assessment of visceral proteins Albumin Transferrin Prealbumin (mg/dl) (mg/dl) (mg/dl) Adequate stores 3.5 – 5.0 212 – 360 18 – 45 Mildly depleted stores 2.8 – 3.4 150 – 211 15 – 17 Moderately depleted stores 2.1 – 2.7 100 – 149 11 – 14 Severely depleted stores<2.1 <100 <10
Caloric Requirement Step – 1 Harris-Benedict equation • Male : BEE (Kcal/day) = 66 + (13.7 x Wt) + (5.0 x Ht) – (6.7 x age) • Female : BEE (Kcal/day) = 655 + (9.6 x Wt) + (1.8 x Ht) – (4.7 x age) Weight- in kg, Height- in cm, Age- in years
Caloric Requirement – kcal/kg Standards • Non – ambulatory/ sedentary patients : 20 – 25 kcal/kg body wt. • Critically ill patients : 25 – 30 Kcal/kg body wt. • Hyper metabolic patients : 30 – 35 Kcal/kg body wt.
Protein Estimation Adult/ ConditionProtein Requirement(g/kg ideal body wt.) Healthy 0.8 – 1.0 Geriatric 1 – 1.2 Mild Stress 1.0 Need for protein repletion 1.1 – 1.5 Critical illness/burns 1.5 – 2.0 Renal failure without dialysis 0.55 - 0.6 Renal failure with HD 1.2 Renal failure with PD 1.4
N Balance and Calorie intake Provide sufficient Non protein calories to spare proteins. CalorieNitrogen ratio • Normal 300 : 1 • Critically Ill 100 – 150 : 1 • Protein intolerance 800 : 1
Quick Calculations for Macronutrients and Fluid NutrientPer Day Calorie - 25 – 30kcal/kg body weight Carbohydrates - 50 – 60% of total calories Proteins - 12 –20% of total calories Lipids - 15 – 30% of total calories Fluids - 1ml/kcal or 30 ml/kg body weight
Fluid Requirement • By weight : 25 – 35ml/kg body wt/day • Depending upon age 18 – 65 yrs : 30 – 35 ml/kg body wt/day • By Calorie intake : 1 ml/kcal Limit in • CHF, edema, oliguria, hyponatremia. • Increase if abnormal Gastrointestinal, skin or renal fluid losses. • Consider all sources, intravenous, enteral and oral.
Types of Enteral Formula: • A) Commercial B) Hospital/ Home based • A)Commercial: • I) Standard/ Elemental- • Normal or minimally impaired digestion • Requires absorption • Intact protein, “meal replacement” • 1, 1.2, 1.5, 2 cal/ml • May contain fiber • II) Hydrolyzed/Pre-Digested- • GI compromise • Improved digestion • Protein typically small peptides
III) Disease Specific- • Designed for specific organ dysfunction or metabolic abnormality. • May not be nutritionally complete. • Hepatic, Renal, Pulmonary, Diabetes,Immuno, Trauma. • Evaluate carefully for efficacy and benefit. eg., Hepatic formulas have more BCAA; Diabetic; • Renal. • IV) Modular- • Modified for one or two particular nutrients. eg., carbohydrate in maltodextrin, protein like whey protein.
Characteristics of Enteral Formulas • Osmolality • Important for its role in maintaining balance between intracellular and extracellular fluids. • All nutrients except water contribute to Osmolality of a solution • Formulas with larger proportions of hydrolyzed nutrients have higher osmolality. • AA and glucose have greater osmotic effect than intact protein and starch. Contd…
Characteristics of Enteral Formulas • Electrolytes have a significant effect on osmolality of an enteral solution because of their dissociation properties and small size. • Isotonic formulas (osmolality 280 to 320 mOsm/kg)are better tolerated than hyper – or hypotonic formulas. • The osmolality of enteral formulas ranges from 270 to 700 mOsm/kg and that of liquid medications 450 to 1095 mOsm/kg. Contd…
Renal Solute load • Major contributors to renal solute load – urea, Na, K, and chloride are associated with water loss and may lead to dehydration. • Water requirement in a formula proportionally to its renal solute load. • Important to monitor hydration level of patients on enteral feeding with excessive loss of fluids. Contd...
Hydrogen Ion concentration (pH) • Gastric motility reduces when pH is lower than 3.5, so the pH of most of the enteral formula is above 3.5 pH level which may cause clogging of feeding tube. • Caloric Density • Caloric density of enteral formula varies from 1.0 to 2.0 kcal/ml. • This determines density of the nutrients and also amount of calories received by the patient. High caloric density formula may slow down the gastric emptying rate.
b) Nutritional Components • Carbohydrates • Principal source of energy, provide 30 to 90% of total calories. • Form and compositions of CHO ranges from large molecular weight CHO (starch) to simple sugars mono and disaccharides and contributes to osmolality, sweetness and digestibility. • Large molecular weight CHO exert less osmotic pressure, taste less sweet and require more digestion. Eg :- starch. Contd...
b) Nutritional Components • Oligosaccharides (glucose polymers < 10 units) and polysaccharides (glucose polymers > 10 units) are widely used in enteral formulas. Due to molecular weight it increases osmolality and sweetness. • Disaccharides like lactose are hydrolyzed slowly due to lactase. LF formulas are mostly used. • Monosaccharides like glucose and fructose. They are sweet and hypertonic, ready to digest, but tolerance may be limited by absorptive capacity of small bowel.
b) Nutritional Components • Proteins • Quality of proteins – influenced by EAA composition . Approx 40% of total AA intake must be from EAA. • Formulas for patients with RF have 100% EAA. • Proteins are in 3 forms: intact, hydrolyzed and crystalline free AA. Contd...
b) Nutritional Components • Intact proteins – are whole proteins from food or protein isolates. Require normal pancreatic enzymes for digestion. • Hydrolyzed Proteins – are hydrolyzed enzymatically to small peptide and free AA. • Crystalline free AA and di & tri peptides are termed elemental or predigested formulas they are absorbed directly into blood stream. • Sources of protein – Meat, Egg, Casein, Protein isolates from egg white, Soya.
b) Nutritional Components • Lipids • It provides 1 – 47% of total calories, EFA and carrier of fat soluble vitamins. Standard formulas have approx 30% of fat. • Two forms – LCTs and MCTs. • LCTs are vegetables oil like soyabeans, sunflower etc. and are source of EFAs. • MCTs are rapidly hydrolyzed within the intestinal lumen and are directly transported to the bloodstream eg. coconut oil. • Contraindicated in patients with high level of ketones. • Fat does not contribute to osmolality of the formulas.
Omega-3 Fatty Acid • Essential fatty acids- Omega 3, Omega 6. • In critically ill patients: Omega 6 acts as pro inflammatory and omega 3 acts as anti inflammatory. • Omega 3: 10 – 20% of total lipids. eg., soyabean, mustard, flaxseed oils.
b) Nutritional Components • Micronutrients • Adequate amount of minerals and vitamins are present in enteral formulas. • Some disease specific formulas are low in electrolytes. • Supplementation is indicated in patients fed on nutritionally incomplete or diluted formulas who are on enteral or parenteral feed for a long time. • Water • Normal adult loses approx. 2600 ml daily which should be supplied to patients on enteral feeding. • Their hydration level can be monitored by daily weighing and intake and out put record.
b) Nutritional Components • Fiber • Normal recommendation is 20 – 35gms of fiber /day. • Fiber is represented in enteral formulas as total dietary fiber (TDF). • Most fiber containing enteral formulas contain 4–20 gm of TDF/litre. • Main source of fiber in enteral formulas are soluble and insoluble fiber. • Commonly used fiber is soya polysaccharide which has soluble and insoluble fibers. Other fibers – Cellulose, gum arabic and oats.
Micronutrients • Required in small quantities • Essential for cellular functions • Marked deficiencies occur in severe stress response (Increased losses, inadequate replacement and increased consumption) • Micronutrient support include vitamin and trace elements
Recommended Daily Requirements of Vitamins VitaminEnteral doseParenteral dose A 1000 µg 3300 IU C 60 mg 100 mg D 5 µg 200 IU E 10 mg 10 IU K 100 µg 10 mg B1 2 mg 3 mg B2 2 mg 4 mg B6 2 mg 4 mg B12 3 µg 5 µg Pantothenic Acid 6 mg 15 mg Biotin 150 µg 60 µg Folate 400 µg 400 µg
Recommended Daily Requirements of Essential Trace Elements Trace elementEnteral doseParenteral dose Iron 10 mg 2.5 mg Zinc 15 mg 4 mg Selenium 200 µg 70 µg Manganese 5 mg 100 µg Iodine 150 µg 150 µg Copper 3 mg 1.5 mg Chromium 200 µg 15 µg
Daily intakes of electrolytes during enteral nutrition or total parenteral nutrition ElectrolyteStandard Enteral NutritionStandard Parenteral Nutrition (mmol/day)(mmol/day) Sodium 80 – 100 80 – 100 Potassium 60 – 150 60 – 150 Magnesium 10 – 18 8 – 12 Phosphate 20 – 40 15 – 30 Calcium 20 – 30 2.5 - 5
Monitoring enteral nutrition • Nausea /vomiting • Gastric residual volume • Abdominal examination • Frequency of bowel movements • Biochemical markers
Immuno – nutrition • Glutamine • Major fuel for the enterocytes, immune cells. • Reduces infectious morbidity. • Inhibits bacterial translocation. • Increases intestinal absorption. • Decreases muscle wasting. • Increases muscle mass. • Fastens wound healing and reduces length of stay (LOS) by 27% in ICU and ultimately cost of hospitalization.
Arginine • Several recent studies have suggested that addition of Ag to enteral feeds may improve outcome in critically ill patients, helps in wound healing. • Endogenous synthesis of Ag is limited during serious illness thus Ag is considered ‘conditionally essential’ amino acid. • Combination of Ag and Omega 3 fatty acid for beneficial effects. www.anaesthesia.co.inanaesthesia.co.in@gmail.com