Tracheostomy May 4 th /05
Tracheostomy May 4 th /05. History. Greek tracheo plus stoma (mouth) creation of a opening in the trachea by suturing the skin of the neck to the tracheal mucosa the placement of a tube through the anterior neck into a tracheotomy

Tracheostomy May 4 th /05
E N D
Presentation Transcript
History • Greek tracheo plus stoma (mouth) creation of a opening in the trachea by suturing the skin of the neck to the tracheal mucosa the placement of a tube through the anterior neck into a tracheotomy • Asclepiades in the first century BC described their use for of upper airway obstruction relief Clin Chest Med 2003
History • 18th & 19th centuries Trousseau diphtheria epidemic surge in the tracheostomy performance & technique improvements but Still mortality 73% • 1909 Jackson modern tracheostomy description • 1969 Toy & Weinstein the percutaneous tracheostomy • 1985 Ciaglia percutaneous dilatational tracheostomy Clin Chest Med 2003
Indications • Permanent tracheostomy post laryngectomy • Relief of upper airway obstruction • Rx uncontrolled tracheobronchial secretions • Prolonged mechanical ventilation Clin Chest Med 2003
Advantage of Trach over ETT • Stable airway • Minimize laryngeal injury • Improved pulmonary toilet and oral hygiene • improved patient comfort • potential for speech and oral feeding • Decreased requirement for sedation or restraints • Facilitated ventilator weaning • Shorter intensive care unit stay Clin Chest Med 2003
Physiological changes • Loss of warming ,humidifying & filtering function of upper airway thick secretions • Defective cough & ciliary function Tube induced mucus production increased risk of atelectasis Loss of smelling decreased appetite
Anatomy • Adult trachea 10 -13 cm larynx to carina • trachea slides easily in the cephalo-caudal direction tremendous variability • With neck extension half the length is above the thoracic inlet
Anatomy • Incomplete rings with post membrane • At thoracic inlet trachea dives from anterior to posterior behind the thymus, innominate vein & artery • In the elderly this angle can approach 90 degrees
Anatomy • Approaching the trachea anteriorly in the midline encounters : superficial cervical fascia, crossing branches of the ant. jugular veins sternohyoid and sternothyroid muscles thyroid isthmus 2nd ring level pretracheal fat pad inferior thyroid veins & occasionally a thyroid ima artery
Percutaneous Dilatational Tarch • Selection Criteria Uncomplicated translaryngeal intubation Palpable cricoid cartilage at least 3 cm above the sternal angle Appropriate neck extension Hemodynamically stable FIO2 < below 60% PEEP < 10 cm H2O Clin Chest Med 2003
Percutaneous Dilatational Tarch • Exclusion criteria Distorted neck anatomy head and neck tumors, thyromegaly or scarring Refractory coagulopathy Tracheomalacia Neck soft tissues infection Inability to extend the neck cervical fusion, fracture, or arthritis Clin Chest Med 2003
Cricothyroidotomy • Emergency situation • Most reliable landmark laryngeal prominence • Palpation along the midline inferiorly toward the sternal notch the cricothyroid membrane immediately above the cricoid cartilage. Clin Chest Med 2003
Cricothyroidotomy • The cricothyroid membrane is identified and incised along its inferior border transversely • Tracheal hook is inserted under the thyroid cartilage. • Gentle vertical dilation is to allow passage of a 6 mm or 7 mm tube Clin Chest Med 2003
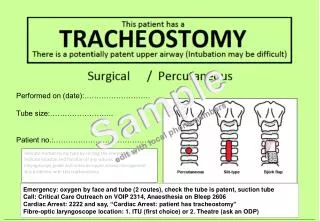
Tube-free tracheostomy • Alternative to tracheostomy tube when it is expected to remain for months to years • To avoid the morbidity associated with an indwelling tube • horizontal omega-shaped skin incision extending beyond the margins of the sternocleidomastoid & arching to the level of the cricoidcartilage • Creation of a muscle & tracheal flap Clin Chest Med 2003
Tube-free tracheostomy • Subplatysmal flaps inferiorly manubrium laterally beyond the sternocleidomastoid superiorly hyoid bone. • Thyroid isthmus is divided the two lobes mobilized to be sutured gathering the accompanying strap muscles & tendons Clin Chest Med 2003
Tube-free tracheostomy • Anterior tracheal flap elevating the 2nd & 3rd tracheal rings • The stoma is intubated until the patient is stable and breathing spontaneously decannulated. Clin Chest Med 2003
Minitarcheostomy • Matthews and Hopkinson in 1984 • novel, minimally invasive method to facilitate endotracheal suctioning and clear secretions • 4 mm cannula through cricothyroid membrane • trachea can be stimulated by a catheter to produce a cough to clear secretions. Clin Chest Med 2003
Minitarcheostomy • preservation of glottic function, secretions can be coughed up via the normal route • Speech and swallowing are unaffected. • The cannula is capped when not in use Clin Chest Med 2003
Minitarcheostomy Indications • Prophylactic Postop major thoracic or upper abdom Sx Extubated pts with expected poor cough Therapeutic sputum retention pneumonia, COPD exacerbations major atelectasis (usually postoperative), depressed LOC thoracic trauma Respiratory muscle weakness. Clin Chest Med 2003
Minitarcheostomy • The success rate 96% to 100% • The average duration of use 1 week • There were no late complication 1-4 y • 2 small RCT post pulmonary Sx 30 & 25 Pts Decrease in post op atelectasis & pneumonia & need of bronch J Thorac Cardiovasc Surg 1991 Eur J Surg 1991
Trach Tube selection • Diameter The smallest outer diameter tube will minimize the risk of tracheal stenosis The widest inner diameter decrease airflow resistance Size 8 men & 6 women. • Inner cannula safe & simple cleaning Clin Chest Med 2003
Trach Tube selection • Cuffed tube mechanical ventilation • Uncuffed tube off ventilator to decrease work of breathing • Wire-reinforced tube enforced security & position tube Clin Chest Med 2003
Trach Tube selection • The fenestrated tube spontaneously breathing pt for easy phonation with the tube capped can be blocked with cannula for ventilation High chance to be blocked by secretion , blood or granulation tissue needs changing frequently Clin Chest Med 2003
Trach Tube selection • Tight-to-shaft Bivona tube intermittent ventilation high pressure, saline filled balloon when deflated is flush with the tube without inner cannula • One way speaking valve Allow phonation exhalation through vocal cord Clin Chest Med 2003
Decanulation • Fenestrated tube cuff deflated cuffless tube • Downsizing progressively smaller size tubes Allows the stoma to gradually fill in around the tube. • Decannulation plug • Tube removal dry, sterile dressing
Complications • Early Bleeding , pneumothorax, SC emphysema pneumonia , Injury to recurrent laryngeal nerve Trachoesophageal fistula Accidental extubation • Late Tracheal stenosis , Tracheomalacia Skin breakdown Cuff rupture or herniation
Should we trach more Pts ? • A lot of studies still no solid answer • Different patient populations • Different timing of tracheostomy • Different surgical techniques & experience
Early Vs late Trach in Burn Pt • Prospective Randomized controlled 19962000 • 21 pt early Trach ET Vs 23 trach D 14 • Predicted probability of prolonged ventilation formula • 1ry outcome hospital stay & mortality • 2ry outcome extubation rate , oxygenation & pneumonia rate Jr of Burn Care & Rehab 2002
Early Vs late Trach in SICU Pt • Retrospective 2000 2002 • Early trach < 7 Vs late > 7 days • Outcomes mechanical ventilation ,VAP , ICU & hospital stay Am Jr of Surgery 2005
Early Vs Late Trach in Head Injury Pts • 2 y prospective randomized study • Early 5th or 6th day Vs late • Isolated severe head injury • Admission GCS < 8 • Cerebral contusion on CT scan • GCS score 8 on the fifth day without any sedation • Outcomes : ventilation , VAP , ICU & hospital stay Trauma 2004
Surgical Vs Percutaneous Trach • Few RCT • No mortality difference • Time advantage for PT less prep time • Shorter time from required to be done • PT may have lower bleeding rate Anaesth Intensive Care 1999 Chest 2000
LMA instead of ETT in Trach • Randomized prospective 60 pts • Bedside trach with brocoscopic aid • Outcomes : procedure time oxygenation & ventilation complications Intensive care med 2002