Download
1 / 31
320 likes | 516 Vues
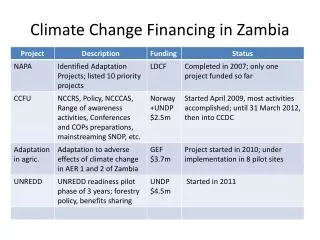
Health Financing and the National Planning and Budget Processes Solomon Kagulura WHO Zambia. Health Financing: global perspectives. Mismatch: health needs & health spending. Projected. What percentage of GDP is needed to finance a health package of US$34 per capita for the whole population?.

E N D
Health Financing and the National Planning and Budget ProcessesSolomon KaguluraWHO Zambia
Projected What percentage of GDP is needed to finance a health package of US$34 per capita for the whole population?
What percentage of GDP is needed to reduce U5M to the MDG target given the impact of GHE between 1990-2000? Assumes a 1% real growth in GDP/capita per year, 5% reduction in illiteracy, 5% increase in road network, 5% increase in sanitation, 5% increase in donor funding
Better process helps win bigger budgetsAnd hopefully better outcomes • In Mauritania, the Ministry of Finance increased the health budget by 40% in 2002. • It was influenced by MTEF analysis suggesting targeted increase would reduce infant mortality by 30% and maternal mortality by 40% in five years. • In Rwanda a similar process led to increased health budget from 6% of total government budget in 2004 to 10% in 2006.
The process graphically: Macro / Sector Links Cost Sector Plan (Health + others) Cost PRSC MTEF PRSP Macro + Financing Constraints Different scenarios
Fiscal space: financing public expenditure in a prudent manner Fiscal space: “availability of budgetary room that allows a government to provide resources for a desired purpose without any prejudice to the sustainability of a government’s financial position” The budgetary resources allocation for health depends on: • Government’s overall fiscal policies • Demand of competing sectors • Spill over effect from one sector to another Fiscal space can be generated through: • Tax measures or improving tax administration • Reallocation of resources away from lower priorities • Borrowing internally or externally • Seignorage • Grants
Fiscal Sustainability Fiscal Sustainability refers to: “the ability of government to sustain spending on a desired purpose for its planned duration, and to meet the cost of borrowing without compromising the government's financial position” Three conditions: • For expenditures funded by loans: financial returns generated by additional expenditure should cover the cost of borrowing • For recurrent expenditure funded by donor grants: if intended to continue these expenditures beyond the planned period of donor funding, governments must be able to raise alternative source of revenue to replace donor funding when it is phased out • For all investments: governments must be able to cover recurrent costs of any new capital investment, e.g. operation and maintenance cost of new health facilities Health sector spending presents particular challenges in relation to all three conditions.
One way is through growth Note: Some Countries Spend Less Than Expected on Government Health Programs
Will Growth Help? Future GDP Growth Will Be Modest Source: World Bank, Global Economic Prospects and the Developing Countries, 2004
Tax revenue is low in SSACentral Government Revenues, Early 2000s Average
Countries in SSA have low tax base a low capacity to increase tax and non tax revenues
EXPANDING GOVERNMENT EXPENDITURES IN HEALTH 80 above regr. line Eritrea 70 below regr. line Quadrant IV 60 Angola Quadrant I Zimbabwe 50 Solomon Islands Lesotho govt. exp. as % GDP 40 Mongolia Ethiopia Zambia Comoros Central African Republic Guinea-Bissau Gambia, The Uzbekistan Yemen, Rep. 30 Togo Burundi Ghana Sierra Leone Burkina Faso Papua New Guinea Congo, Rep. Mali Niger Moldova Benin Malawi Tanzania Sudan Pakistan Azerbaijan Kenya Georgia Mauritania Rwanda Indonesia Vietnam Senegal Kyrgyz Republic Cote D'Ivoire Bangladesh 20 Chad Tajikistan Nepal Madagascar India Guinea Cameroon Uganda Nigeria Equatorial Guinea Congo, Dem. Rep. Haiti Cambodia 10 Quadrant III Quadrant II 0 0 3 5 8 10 13 15 govt. health exp. as % govt. exp.
But government spending has its limits Assumes: Past impact of GH on outcomes remains constant and that, GDP per capita, donor funding, road network and sanitation coverage increase at 2.5% per year. Illiteracy is assumed to decline at 2.5% per year. Donor Funding is assumed to be only 1/3 as volatile in 2015 as in 2000.
Donor funding • Donor funding is relevant mostly in Africa a few other LIC • Meeting commitments is proving to be difficult • Most Donor Funding for health comes in the form of vertical programs and is off budget • Recent econometric work shows that additional donor funding does no have an impact on U5M and MM unless volatility and fungibility issues are addressed The following charts illustrate some of the problems
Donor Funding: Are commitments being delivered? ODA is Rising But is Far Short of What is Needed to Meet the MDG (0.54) and the Monterrey Commitments (0.70) Prospects for ODA in 2006 and 2010 are based on DAC members’ post-Monterrey announced commitments. Not all DAC members have made commitments beyond 2006. Source: OECD DAC database.
A Large Part of the Increase in Aid is Not Directed to Financing the Incremental Costs of Meeting the MDGs Increase in ODA is concentrated in • debt relief and TC • a few countries Breakdown of total increase in nominal net ODA of $16.7 billion in 2001-03 The real increase in ODA in 2001-03 is $7.5 billion in 2003 dollars.
Where Does All the Aid Go? • On average, for every $1 disbursed by donors to our 14 case study countries, we estimate: • Not recorded in balance of payment $0.30 • Recorded in B of P but not in Govt spending $0.20 • Aid earmarked to specific projects $0.30 • Budget support $0.20 • 1990s structural adjustment provided a larger share of aid as general budget resources.
Conclusions • Countries are behind with respect to the MDG goals • Broad agreement exists on health priorities. • Accountability for results is not always supported by control of the resources necessary to achieve them. • Fiscal constraints are binding, particularly in low-income countries. • Public health expenditure needs to be well- targeted and allocated to high impact interventions proven to work.
Conclusions • In good practice cases, PRSP identifies spending priorities in consultation with sectors, MTEF/budget process shifts resources towards them, reviews and adjusts each year in light of performance. • Capacity problems can be managed if bottlenecks are tackled in a logical sequence, avoiding large "earmarked" commitments that distort priorities. • Progress to the MDGs requires more budget support in aid-dependent countries