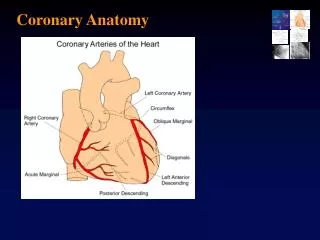
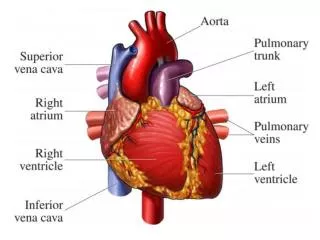
Coronary System
Master key glossary terms, manage arrhythmias like bradycardia and tachycardia. Learn nursing care for angina and myocardial infarction. Understand coronary system intricacies and cardiac medication protocols for optimal patient care.

Coronary System
E N D
Presentation Transcript
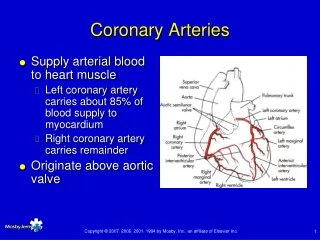
Coronary System • EO 1.1 Read and master terms in glossary • 1. Normal Sinus, the normal conduction pattern of the cardiac cycle which originates in the SA node. • 2. Arrthymia; Any deviatin from the normal pattern of the heartbeat • 3.Bradycardia; Abnormal circulatory condition in which the myocardium conducts steadily but at the rate of less than 60 contractions a minute. Possible causes; intra cranial pressure or digitalis toxicity.
Coronary system • Bradycardia; trxt may include adm. Of atropine, pacemkr., or red. In dig. • 4. Tachycardia; abn, circul. Cond. .100bpm • The d/c rate from the sinus node is inc. as a reslt of vagl inhib.
Nursing Mngt of Angina • 1, obt full des pain., quality, radiation, aggr, and elev sym, n/v, triggers. • 2. check v/s bp, resp rt. \\ • 3, check; rate, rhtym, ect hrt sound, look for arrythm, Abil to inti card impls, SA node initiator,,S3 soft low pitch after S2, poss. HF /S4 low pitch b4 S1, vib of atrial wall by diastole, vent. Less compliant. Listen for murmur,don’t contract during sys. Goes into left atrium, lft sys murmum • Ask about dysp, assess breathing, note crackles, p • Prep pt for tests, 12 ld ecg(isch, inj, infac, t waves ,look for lipid profile, CEZ, CkMB creatine kinase, lipid pro, show hyperlipidemia, trigy, hdl,ldl, vldl,
Coronary • Ldl,vldl form choles 200mg/dltri, tri.160,ldl.180 • Hdl trpst choles to liver • CAD • Stress test, Inc O2 demand, ,or inplace of exec., dipyridamal,
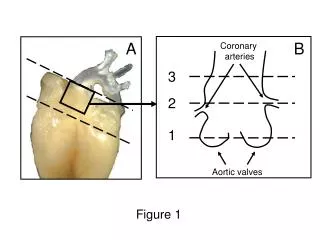
Coronary Angiography • Dyes inj into l an r art, able to see blck in branches • To confrm, rev rslt with dr, then pt. • # art efftt, pt resp to trsxt, pt may need drg, surg, or both, • Poss. Just 80mg of ASA, inhib thomboxine, I • Lipid redc. Agents, • Vasodialtors, Nitrates, • CA blcks, dialate cornry art. Low O2 demnd, and aftld • B adrn blcker, dec hr, myo contrct, use less o2 at rest
CAD • Heprin, prvt fibrgn to frib • Intra aortic balloon pump, temp • > 2,3 arteries, Ptca, • Arthrectomy • Coronary stent, mesch with balloon • Left dis, use bypass
Nurs care • 1. adm O2 • 2 est, main intrv access, ie nitro, hep • 3 freq v.s • 4 ascultate brth snds • 5 check ECG mon, 12 lead, rest of bld test for abn levl
For DC Nurse to do • 1 rev inst about drgs, dose freq se • 2 act consr • 3 lifestyle mod • 4 signs and sym • 5 follow up care
Nursing Lecture • Goal of MI dec, act, do for them • Angina • Dig find • 1 Hx P • 2 Cardiac Eng • CPK • LDH • SGOT • CPK MB ISO Enzymens • 3. EKG Chngs • !Q wave • ST seg elevation • T wave inversion • 4 Dysrhythmias • 5 Increased Temp and WBC
Dignostic findins • Use Nitro at home and if nitro doesn’t work go to hosp to adm strptokinase within 6 hrs of MI • In a MI very severe crushing severe chest pain, bld is divt away from skin, cold sweat, grey in color, as bld is shunted away from periphery, Jaw, down left arm and to the back • If nitro q5min x3 doses relieves pain it is prob angina • If pain not relieved then it is probl a MI • Trxt, O2, • Sym are very dramatic, suffocating pain, Elv HOB, start IV therapy, key is to reverse pain (then you are controling ishemia)’, 12 lead EKG, comp is dysrythmia, #1 comp Vent Dystrm with 1st 24 hrs, • Blood work orderd, CPK, and if elev do CPKMB, or CKBands
Digan • Total CPK if not elve do not do iso enz • If elev do fraction of isoenzyme, BrainBB, heartMB, and skeletal muscleMM, to identify • CPKelev up to 4-6 hr on the onset of the event • Troponin/quiker than CPK X3 for 1st 24 hrs or q8 and if elevated client is trxt as a New MI • Myoglobin not spec but elev quickly just that musl tiss dmage • Get E-lytes, K, & Mg • Choles/lipid profile, to assess for risk factor • Glu to find undigansd diabetes • Thyroid stud, due to abn. Fat in thry action
Cardiac meds • Dysr most common compl due to occurnc in lft vent. • Cardiogenic shock; the myocrdu is so damgd cant perform tissue perfusn, gret deal of vetn destryd., ist symp; • Confusn • Dec loc, chngs in urine output due to dec tiss per, cool moist clamy skin • As body decompensate, hypotension, brady, but initial you have hyper/tach
Cmed • Lasix/bumex loose K • Anticoag; heprin drip/if you intrven quickly you want to dec plat agg and prevt ext of blood clot , the only ones sthat will brk it down is strptokins, but to prnvt closer use hep drp, and after strpto prcd to prevt reclsr. • Client at hight risk, put on low dose hep 5000 u bid sq, or lovenox, due to allegeric rxn to hep, given based on wt. Give inch around umbilicus. DO NoT asp or masg area. • If clint asks about dose, tell the they hav a chng in act level, ie bedrest, to prvt clots. At home they would be on coumadin
manga • We can give Nitro, sling, or run a nitro drip is chst pain unrelved with nirto sling, as paste is used for mang or acute episds of chest pain, so it is very rapid on set revesr myo car ishch. • If chest pain cont give mcg per minute of nitro. Usually 10mcg per minute for chest pain to titrate drip. • Give MS for cardiac client/drug of choice/has advngts, dec anxiety,CNS deprst, slow hypervetn and RR, relv Cest pain, and good give q15min 2-3mg IVP and repeat for pain releif. And dec preload and afterload(dec myo O2 demand ,Hrt doesn’t have to pump as hard) which is why they get low BP so monitor BP. • Nitrates also dec prelod and aft load
Beta Blck • Always give as protocal: Lopressor • Beta Bcks and Nitrates to dec injury, pt are prophylatically placed on both. To save myocardl tissue. • So when the client comes in put them on telemrty/o2/meds • If its anginal pain alone, nitrats will work if not give IV drip
Pharm inter • Know drug; know nursing actions Key • Nitrates; Maintenance or quickly revsr pain, • Transderm nitroderm 24hr rels patches, take off at night due to ptl develp tolerance to nitrates. • Isordil: long acting,Indur, Nitrobid use for Maintenance. • For quick relf, transdermal, iv
Med vasodialator • Nitrates;vaso dil; dec preload venos ret, dec O2 demand on heart. • Dec on aftrld, look to where blood is being ejct to arterial, antihypertensive meds, ca blcks, ace inhiber • Nitrt/MS dec preld and aftrld Nitrts vaso dialates incr cornary arety, SQ given q5min x3, and q5 get BP,hr, and ask if pain is relieved, keep asking, big side efft, HYPOtension, terrible headache. They evently develp tolerance, You may also see, mild reflx tachycarda, body tries to incr tissue perfusin,
Meds • Beta adrendergic blcks. B2 in airway, sitm casu brocnh, We use Beta agonist in resp, but B1 spec to myotissue, beta recp in • Beta blck dec hr, dec forc of cont, incl lung cause vaso constrct, so you hav to evea brthing, if you dec hr, cardia out put goes down, • They can cause HFailure and it quite in d/c teching • If Hr less than 60 do not give , • You can not just tsp e beta blcke you get ince cardica demp and anginal pain, let the dr, know that hthe hr, is 53 or 54 as long as they arenot symtomatim
Beta blcks • Have a secdy efft by dec renin production,,will give you dec renal perfussion,so it builds up, not good so in CHF if you have excessive renin you worsen the whole syndrome, rembr, if aldostrn is rels, it inc Na and h2o, and dec K, you will worsen CHF,, Renin also is dec in anti anxiety disorder, in psych can be given to dec aggression, becs renin is relsed as stress respsn. Dec anx and agitation, sign risk factor is ANGER!!!! Not just type A any more
Beta blcks • Bradycard • Hypotens/due to renin dec • Wheezing, obst in lung • Depression • Sexul dist/ sexul impotency
Beta blck • Used to sslve myocardiund to dec afterld, dec BPm, keep pt out of CHF, but get excess red in cardica wrk lod, if they are on three it can cause CHF • Ca blcks are used for heypr tension and corrary arty spsms. And some Verapimmil, or Klany, or Carizem for vent Dysmy, • They tend to slow the heart, so the efftect the SAnode and AV node to slow elec condu, and dec dysrytmis • They blck the inflx of Ca into the tissue in the velles or byo, you dec vasoconstr and force of contrct, and dec aorny spsm • Sys dial=BP • Slow hr = red myo demand can cause HF
DC teaching for client • Report Wt gain weigh qod, not over 2-3lbs rept to dr. • Look for signs and symp legs swelling, shoes too tight, legs feeling heavy, rept to dr. excess fatigue, unexpl cough, dysepna, SOB with act that last week didn’t produc that • Evidence of Acites= abd distension • Teach how to take BP, if they are holding fluids their systolic will be higher • Diet, avoid hvy meals, fat, emotionl upset, if they know they have to do something strenusos, take NT prior to excecise • Use cardiac rehab, learn to space activty • Possl cardica cath
Meds/DC tching • MS/ASA/ativan/xanax • Choeslerl lower agent ,levocor, prevacol,lipitor,crestor(liver dec LdL, but can inc HDL)prevents progression of atherorschlers • Chol manu in liver, main side effect of choels lowering agent you get liver damage, teach them to look for sym, jau fullness, tenderness, acites,jundice, abd pain upper quad, can cause brkdn of muscle, rept to dr. place on low na low choles high sodium foods are process foods,teach them to read labels
Teaching/procedures • Angioplasty/or PTCA • CABAGE • Ethrectomy go in with tiny blade or laserand shave away plaque. • If client doesn’t chang lifestyle they come back, so there has sto be a lot of lifestyle changes, Nurse must use motivational teaching, • Pat should be follwd up by cariologys and go to rehap, • Client can go back to sexual act with 1 wk after uncomplicated MI • Healing time is from 4-6 weeks, stages, ischmeia, injurgy, then necrosis • Alt,ASt,LDH, in system for 6-8 days, if a pat has had chest pain for 1 week they can remain high, if EKG is showing damage use old enzymes.
CHF Definitions • Know basics/and how to trtx patient; • Defined faiur of hr to meet met and o2 edemp of body, unable to meet or maintemn tissue perfusion • Remebr take yers, most cleitn have had this prbl for som time • CHF evlovs ofve time, you can have acute CHF with excacebation but rare onset immediated
CHF • Pregnancy last trimetsr • Cocaine • Typical pt has compensatory mechisn • Vent dilation, use echo to see chamberrs of hert, so there is lenghtn of muscl fibe • Vent hyperthrph(thcking of wall, hrt works hrder musckle tnd to ticken,same as wt trainger, get thingk of ventirkcal wll, andof failu but s it cont th can keep pt out • Tachycardir hrt out grow, or caddio megghalybecoes a boggy herts the blood suply, so it • Renin release ,,relsed in resp to BP, or cicul Bld volum, there the kndy are undr perfused, and renin is reldsd and bloodkis hsunted asway from kindly and all it does is worsen fakil, pt hangs on to , drugs used ACE inhibtors stops angion tension one to angion tension term so the biggest effedt of ACE is lower BP, fld vl decfict,, tachycardy, Kptssum builds up , so watch for hperkalemia, as Na and h2o excet monior serum potassum • body sensses it is iscNA and wather, its ok for the shcck, flud vol dect pat , but not good for cardic pthmeic so it incks hert. Hr not good for cardiac pat. Worsen ishchemi
Aldosterone Antagonist • #Aldactone meds, it is a poticsm sparing diruet meet medtobl d eree • I, temand, left side most common • Eitiogng one , t • Cant efft left without right so you will get syp of both usulay of both but left if the first side, the exceptin is cor pulmoale, so the left side fist
CHF • Appched with hypertension , atherersclesoss, and dysrmty • Ltf side of hrt (if u have damge to left side heart faily blood bcking up tform left vet to left atum to lung, and lungs are unable to ocsgent and due to flud or secr in lung • Diag find pulmonaryl conge, or caridomegly • Dilation of venty inc chamer and dec ejection fraction, we want a 40 plus60% less than, so the echo will Ekg, show rt venty hyperthorypty
CHF • Left side preced rth side hrt fail • CXR show congest • Sypm of rt side het failr go from lt vent, to rith vent to systemic • Signs and sympt • A.fatigue, • Distended jug • Ascites, liver becks engored heptomegal, • Inc perifpevenou presso • Anorexid and c/o gi deistress, due to all sys engorgemtn • Fatiugue is prestn in both lt fna dfrith side hrt fail • Wt gain, teach pta to reptort symp
Lt side • Left vet, left atruim, pulmony vasucaltou • Prarosc noct dypssnes • Confusion • Leve pul caplif wedge press, • Cough • Crcke • Orhtermeon • Tahccare • Wheezine bllod tinge sputem frothy (dangerouw • en • restl
Signs left side • All pt exist in a comeing pete, and then a stsressor thows them ofver the edge, • or some will stop taking med/ stated temp ext, diatry, ate too much, don’t have the money for meds • Restlessless, tach cyanossi confusion
Patient with MI • Alrdy have a damgd Hrt • Must monitor for the extremes
Describe pain • Typical • Mowing lawn, got SOB, sat down and got Real sweaty and got pain across chest • What do you do to releive pain,? • Take nitro, O2, how do they • HX and risk factors, medication at home lopressor, cordorn, nitro, avandia, glucophage, astshma inhaler
With 24 hr Inc WBC and inc Temp • Immune resp set up due to inj • Management; if a pt comes in with cardiac pain give not only nitro but ASA as well. 325,281, 162, low dose, (dec viscosity and incr myocardial perfusion