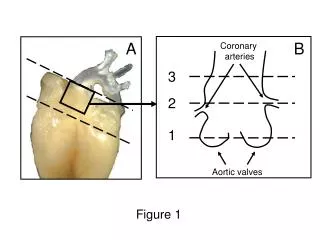
Coronary Anatomy
Coronary Anatomy. ½ Loop and Circle. ½ L oop – L AD and PDA C ircle – RCA and C irc. Right Coronary Artery. Rt A.V. Sulcus 85% Rt dominant 7-8% Balanced 7-8% Left dominant Rt PDA Post Interventric Groove. Right Coronary Artery.

Coronary Anatomy
E N D
Presentation Transcript
½ Loop and Circle ½ Loop – LAD and PDA Circle – RCA and Circ
Right Coronary Artery Rt A.V. Sulcus 85% Rt dominant 7-8% Balanced 7-8% Left dominant Rt PDA Post Interventric Groove
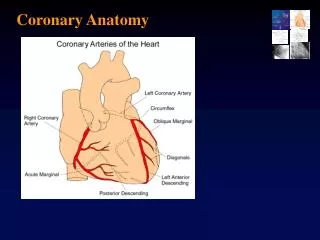
Right Coronary Artery The RCA arises from the anterior right coronary sinus somewhat inferior to the origin of the LCA. The RCA passes to the right of and posterior to the pulmonary artery and then downward in the right atrioventricular groove toward the posterior interventricular septum. In more than 50% of individuals, the first branch of the RCA is the conus artery, unless it (the RCA) has a separate origin directly from the right coronary sinus. The second branches usually consist of the sinoatrial node artery and several anterior branches that supply the free wall of the right ventricle. The branch to the right ventricle at the junction of the middle and distal RCA is called the acute marginal branch. The distal RCA divides into the PDA and posterior left ventricular branches in a right dominant anatomy RAO Lateral
Left Coronary Artery Lad - Ant Intervent Groove Circ – Post AV Groove
Left Coronary Artery The Lt Main arises from the left posterior coronary sinus, is 5–10 mm long, and does not vary in diameter. The LCA passes to the left of and posterior to the pulmonary trunk and bifurcates into the LAD and LCx arteries. Occasionally, the LCA trifurcates into the LAD and LCx arteries and the ramus intermedius. The ramus intermedius has a course similar to that of the first diagonal branch of the LAD artery to the anterior left ventricle. The LAD artery passes to the left of the pulmonary trunk and turns anteriorly to course in the anterior interventricular groove toward the apex. It provides the diagonal branches to the anterior free wall of the left ventricle and the septal branches to the anterior interventricular septum. The LCx artery courses in the left atrioventricular groove and gives off obtuse marginal branches to the lateral left ventricle. In a left dominant or codominant anatomy, the LCx artery gives rise to the PDA or posterior left ventricular branches
High Takeoff of Coronary Artery Usually Asymptomatic 6% of Hearts
Of 126 nontraumatic sudden deaths in young adults, cardiac abnormality was found in 64 cases (51%), with coronary artery abnormalities being the most common cardiac abnormality 39 of 64 patients (61% )
Multiple Ostia Typically either the RCA and the Conus branch arise separately, or the LAD and LCx arteries arise separately with no Left Main (0.4%)
Separate origins of right coronary Artery and conus branch An aberrant conus artery arising separately from the RCA is particularly at risk for injury from ventriculostomy or other maneuvers performed during heart surgery
Single Coronary Artery Single ostium from the aortic trunk Extremely rare - seen in only 0.0024%– 0.044% of the population A single coronary artery may either follow the pattern of a normal RCA or LCA, divide into two branches with distributions of the RCA and LCA, or have a distribution different from that of the normal coronary arterial tree Although a single coronary artery may be compatible with a normal life expectancy, patients are at increased risk for sudden death if a major coronary branch crosses between the pulmonary artery and the aorta. In addition, proximal stenosis of a single coronary artery may be devastating if there is an inability to develop collateral channels Rt Coronary arising from LAD
Rare Follows Lad or RCX High risk if Anomolous course Poor collateral flow Single Coronary Artery Low Risk RCA (Curved) arises from Lad (Straight)
Single Coronary Artery High Risk Due to Pre- Aortic Route of RCA
Multiple Ostia Typically either the RCA and the Conus branch arise separately, or the LAD and LCx arteries arise separately with no Left Main (0.4%)
Coronary CTA Technique Heart rate approx 60 or less Non contrast first for cardiac scoring NTG prior to injection 80 cc contrast followed by 40 cc NS flush Scans reconstructed at various stages of cardiac cycle 70-80% best…late diastole 30% 40% 65% 75%
Anomalous Origin of the Coronary Artery from the Pulmonary Artery (ALCAPA) • One of the most serious congenital coronary artery anomalies. • It has an estimated prevalence of one in 300,000 live birthsMost affected patients show symptoms in infancy and early childhood. • Approximately 90% of untreated infants die in the 1st year of life • Most common form- the LCA arises from the pulmonary artery and the RCA arises normally from the aorta (Bland-White-Garland syndrome) • Coronary angiography demonstrates collateral circulation between the RCA and LCA and a coronary “steal” • Treatment of ALCAPA consists of re-creation of dual coronary perfusion. • Infantile ALCAPA, either • direct reimplantation of the anomalous LCA into the aorta or • creation of an intrapulmonary conduit from the left coronary ostia to the aorta • In adult type ALCAPA, ligation of the LCA from the pulmonary artery, combined with coronary artery bypass grafting with use of the internal mammary artery or the saphenous vein
ALCAPA Pre- Op (Bland-White-Garland Syndrome) Enlarged Rt. Coronary with collaterals to LCA RCA off Aorta..LCA off Pulm Artery
ALCAPA Post- Op • LCA tied off from Pulm Artery • Lt. Int. Mammary Artery connected to LCA • RCA smaller • Collaterals Less
Origin of the Coronary Artery or Branch from the Opposite or Noncoronary Sinus and an Anomalous Course It has been postulated that, when dilation of the aorta occurs during exercise, the anomalous slit-like ostium for the RCA in the left sinus becomes narrower, possibly limiting coronary blood flow and resulting in myocardial infarction Intra-Arterial (A) has a high risk of sudden cardiac death Anomolous Rt. From Lt Sinus most commonly follows intra-arterial course with 30% mortality
Anomolous Coronary Origin Anomolous Rt. From Lt Sinus most commonly follows intra-arterial course with 30% mortality Intra-Arterial (A) has a high risk of sudden cardiac death
LCA arising from RT Sinus with Pre-Pulmomic Course Usually low risk
Myocardial Bridging Myocardial bridging is caused by a band of myocardial muscle overlying a segment of a coronary artery. It is most commonly localized in the middle segment of the LAD Compression of LAD during systole Can cause Sudden death May need systolic reconstruction to visualize
Left Circumflex arising from RCA Retroartic
Coronary Artery Fistula 0.1% of Pop RCA>LCA Coronary artery fistula is a condition in which a communication exists between one or two coronary arteries and either Cardiac chamber RV 45% LV/LA 10% RA 25% Pulmonary artery15% Coronary sinus Superior vena cava <5% Lt side mimics Aortic Insufficiency Rt. Side left to right shunt May lead to ischemia
Corrected Transposition Coronary arteries originating from both aortic sinuses. Note that the aorta (A) is located anterior to and to the left of the pulmonary artery (PA). The ventricles with their respective atrioventricular valves (not shown) were inverted; thus, the distribution of the coronary arteries is reversed, in keeping with the ventricular inversion. The anterior aortic sinus corresponds to the noncoronary sinus. The morphologic LCA (white arrow) arises from the right posterior aortic sinus and supplies the pulmonary ventricle (anatomic left ventricle). The morphologic RCA (black arrow) arises from the left posterior aortic sinus and supplies the systemic ventricle (anatomic right ventricle).