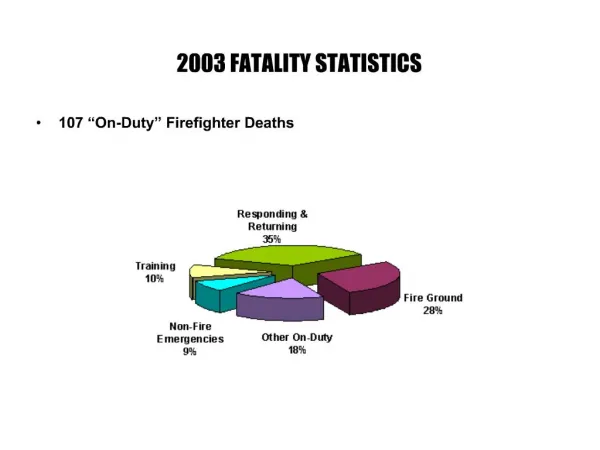
Fatality Review
Fatality Review. The illustrations in this presentation are explanatory aids and should not be regarded as graphically exact technical representations. The questions (reflections) are designed to prompt discussion and may not be in any way related to contributing factors to these fatalities.


Fatality Review
E N D
Presentation Transcript
Fatality Review The illustrations in this presentation are explanatory aids and should not be regarded as graphically exact technical representations. The questions (reflections) are designed to prompt discussion and may not be in any way related to contributing factors to these fatalities.
Between 2000 & 2002 there were 11 Fatalities on Offshore Installations in the UK, Norway and Holland. These were our friends and colleagues We need to work together to make sure that we have no more deaths in our industry How will you be making your next trip home?
No 1 Jan 2000 A B • Reflections • This is how the joint was slung. How do you sling pipe? • If you saw this, what would you do? • Would you be happy to stand under this (or any) load during a lift? C The Event: Man struck by joint of casing: The sling slipped up the pipe [A], the casing swung down and outward [B], hit the deck, bounced and struck a man standing on the deck [C]. This fatality involved lifting.
No 2 May 2000 • The Event: Man struck by a 3Ton bundle of pipe as it was moved onto catwalk. This fatality involved lifting. • Normal practice was to remain in the ‘bus-shelter’ (yellow area) as loads were moved. • The crane driver had just been relieved for a meal by the assistant. • A tool-box talk was held at the start of shift – but not for this changeover. • Reflections • This is a routine task – some of our routine tasks carry significant risk – why? • Do you get comfortable with routine tasks – eg crossing a busy road?. Perhaps we are far less at risk in unfamiliar operations where our guard is up?. • Do you have enough safeguard built in to allow a momentary lapse of concentration? • What is the quality and frequency of your toolbox-talks?
No 3 Oct 2000 • The Event: Man Crushed. • A man was working on the control hoses for the diverter under the drill floor – suspended on a man-riding winch. During the operation, the man was raised too far and crushed against the bottom of the rig floor. • The man operating the winch on the drill floor was unable to see the man in the riding belt. A radio was in use between the man on the winch and a banksman on the BOP deck below. • There was no safeguard against the communication failure. • The manriding winch was capable of generating large loads. • Reflections • Do you carry out manriding operations? • Do you use the Step Change guidelines and signals? If not, are your own systems as good or better?. • Manriding is a bit like flying – if you or your family are in the air what expectations do you have of the pilot (winchman), air traffic control (banksman) and passengers (the man in the belt)?. • Do you carry out operations that rely on radio contact – how to you ensure that radio failure does not lead to death or injury?
No 4 Dec 2000 The Event: Man struck by bundle of drillpipe: Two men (blue basket) asked the crane driver to lift out a tool & move the basket. The deck had a blind spot (see drawing), caused by the pipe shuttle. The crane driver went to do the lift and realised that he needed to move pipe to make room for the basket. In the meantime, unknown to him, two different men came into a nearby basket. While lifting the bundle of pipe (without taglines or a banksman) the bundle started to rotate and was set down next to the blue container in the belief that the two men visible were those who had requested the lift (ie that the blind spot was clear). One of the men managed to jump to safety, the other was killed. This fatality involved lifting. • Reflections • What rigorous precautions do you take for blind lifts?. • What lifts can you carry out without a banksman? • On your installation, are banksman duties clear? • Is this a routine task (routine= usual, common, regularly carried out …). If so does that make it safer? • Could this happen on your installation?
No 5 Mar 2001 The Event: Man fell through hole to lower deck. A jack-up was working over a small platform. The normal solid hatch had been replaced 10 days before with a ‘drilling hatch’ with a 42” hole. This was covered with a plate, 5 sleepers and surrounded by a scaffold barrier. The crew reached the stage where access to the well was needed. Three crew members had removed the sleepers and were removing the plate when one crew member stepped in the hole and fell to the deck below. • Reflections • How do you protect such openings on your rig? • How does that protection stretch across shifts or crew changes? • If this accident were to ‘almost happen’ on your installation, would you report it? • If you were to report it – would you class it as high potential (ie a very serious near-miss)?
No 6 Jul 2001 • Reflections • Is this a routine task and if so what dangers does it pose? • What protection have you got against this type of event? • Do those who routinely perform this task consider it routine and perhaps trivial? • Where will the drillers focus be in an operation like this – rotary or elevators? The Event: Man crushed by descending equipment. Picking up and running pipe on the drill floor. As each joint was added to the string a stabbing guide was used on the pipe to protect the thread as the next joint was being added. On this occasion, the top-drive descended considerably more than required; this coincided with installing the stabbing guide. Is this a lifting operation?.
No 7 Nov 2001 The Event: Man fell 37m. A barge supervisor was carried out maintenance on a personnel lift (to change out the rope that raises/lowers the lift). The lift was suspended on slings supported on a piece of pipe placed across the aperture of the winch housing floor. The man was standing on top of the lift, when the pipe supporting the lift moved and the elevator plunged to the bottom of the shaft. • Reflections • Do you know how lifts on your installation are maintained? • Is this a routine operation? How would you plan for an operation like this? • What secondary measures would you take to protect yourself and others? • This is working at height – what are your procedures for such work? • If you don’t have lifts – what operations on your installation bear similarities to this one? How are they managed?.
No 8 Jan 2002 • The Event: Man fell overboard. • The task was to secure the diverter (red item) on the cart - a small platform over open water. One chain was secure, a ‘cheater bar’ was needed for the other. • The terms of the permit to work regarding life vests, securing the harness and calling in the standby boat had not been carried out by the supervisor. • A “Time-Out” was called for but not taken. • The cheater bar was thrown to the man on the cart (the supervisor), he did not catch it cleanly, rolled over and fell into the sea. He was not found. • Reflections • Supervisors need to care for themselves as well as their people. • Supervisors need to demonstrate the very best safety behaviours. • How rigorously do you observe the terms of the permit to work on your installation?. • If a time-out was called, under what circumstances would you not take it?. Some handrails etc have been removed from this drawing for simplification.
No 9 Mar 2002 The Event: Man Crushed by basket. Offloading a supply vessel. The task was to stack one basket on top of another (dissimilar) basket. The basket was hanging unevenly – one end was higher than the other when suspended. Dunnage (timber) was used to support the upper basket. The banksman went into the bay where the baskets were being stacked with a view (it is believed) to re-positioning the dunnage. While there the basket slipped and the banksman was crushed. This fatality involved lifting. • Reflections • If you stack baskets, are they suitable for it? • Do you use timber as a structural member? • What is the role of the banksman – is it crystal clear on your installation? • Have you ever been asked to act as banksman – are you qualified? • How should one read the risk in this operation and when should one say STOP?. Views looking Aft View looking Forard
No 10 Apr 2002 The Event: Man hit by dropped object. A design engineer was working on a landing frame on the lower deck area (moon-pool) of a drilling rig. He was a visitor to the rig – not part of any normal crew. Normal operations were proceeding on the rig floor using the catwalk trolley. A crossover sub (large piece of pipe) fell through the mousehole opening and hit the engineer below. • Reflections • How do control ‘work below’ on your installation? • How do you manage/control day visitors and their activity? • If you remove hatches, how do you protect people on other levels? • When you remove such hatches – do you immediately think in terms of a risk created? Mousehole. Trolley Landing Frame Crossover Sub
No 11 Nov 2002 The Event: Man crushed by falling tank (chemical pod). Two pods had been stacked and were to be un-stacked. On request the crane driver lowered the crane pendant – it came down too far and fouled between tank and frame. The banksman, while standing on the ladder of the upper tank, made a radio request to the crane driver to pick up 20cm. On doing so (with the ferrule fouled), the tank lifted, slewed sideways trapping and crushing the banksman against an adjoining container. This fatality involved lifting. • Reflections • How do you communicate with the crane driver? • What else are you doing at the same time? • Can you reach lifting equip. on your installation from the deck? • Do you separate the duties of banksman from those who touch (or stand on) the load?. • How well protected is your lifting equipment from fouling on the load?
Common threads identified in the report* were… • Mistaking routine for safe. • Supervisors not spending (or unable to spend) sufficient time on site setting expectations. • Workers vulnerable because they do not perceive risk. • Established Procedures ignored. • Ignoring of Procedure is observed – but tolerated. • Risk assessment cumbersome and not used at the ‘coal-face’. • Lifting Operations. • Banksmen involving themselves in the actual movement of the load. • Some hardware issues – e.g. manriding procedures & kit, cargo baskets. • High Potential near misses are occurring – we need to address them. * Read the booklet “Fatality Report” for more detail.
In conclusion… These fatalities all occurred on drilling rigs. However all Hi-potential near misses are not restricted to drilling. Consider these fatalities in the context of you own installation and bear the following in mind… If we were to address even a few of the common threads effectively(notably lifting operations and the activity of banksmen) the impact would be profound !
Further information is available in the booklet “Fatality Report and in the accompanying CD. Copies of the booklet and CD can be obtained from Step Change in Safety – contact details on the web at www.stepchangeinsafety.net or e-mail info@stepchangeinsafety.net