Download
1 / 23
250 likes | 467 Vues
5 th Arab Radiological Congress of the Pan Arab Association of Radiological. CONTRIBUTION OF MRI IN THE EXPLORATION OF CHILDREN HYPOPITUITARISM.

E N D
5th ArabRadiologicalCongress of the Pan Arab Association of Radiological CONTRIBUTION OF MRI IN THE EXPLORATION OF CHILDRENHYPOPITUITARISM M. ALOUI, N. AIDI, W. DOUIRA-KHOMSI, A. EL GHAZALY, H. LOUATI, L. BEN HASSINE, L. LAHMAR, I. BELLAGHA Department of Pediatric Radiology, BechirHamza children’s Hospital Hammamet, 26-28 April 2012 PED1
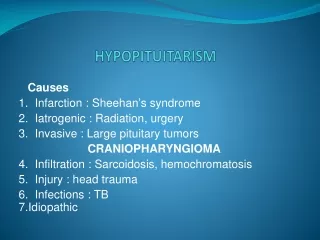
Introduction • Hypopituitarism refers to the absence or reduction in function of hormones produced by the pituitary gland • It may be idiopathic or associated with organic causes, such as tumor, surgery, or irradiation of the sellar area • Early diagnosis and treatment promote the best possible outcomes • Magnetic resonance imaging (MRI)retains an important place in the diagnostic and therapeutic approach of hypopituitarism
Objectives • Illustrate through 14 observations, the contribution of MRI in the exploration of children pituitary insufficiency • Review the role of MRI in the morphological exploration of the sellar region and the detection of the associated brain damage
PATIENTS AND METHODS • Retrospective study involved 14 children monitored for non tumoral-hypopituitarism including 13 with clinical growth retardation and one with hypogonadism. All of them have a pituitary MRI • Patients were admitted to this study only if MRI revealed anterior pituitary hypoplasia
PATIENTS AND METHODS • Technique • MR studies were performed with a 1.5-T(GE Medical System) • All patients were explored with the same protocol at the level of the pituitary • Sagittal and coronal T1-weighted spin echo images • Sagittal or coronal T2-weighted fast spin echo images • T1-weighted sequences after intra venous administration of contrast agent if pituitary stalk was not seen
PATIENTS AND METHODS • The height of the pituitary gland was determined on the midsagittal T1-weighted image by measuring the greatest distance between the base and the top of the gland • Pituitary height measurements were compared with published normal values for age • A pituitary was considered to be hypoplasic when the gland height was less than -2 SD for age
Results • Age range: 2 to 17 years (at the time of MRI) • Sex:8 males, 6females • Absence of family history of hypopituitarism for all patients • Hormonal assessment • Isolated Growth hormone deficiency (IGHD) in 8 cases • Multiple pituitary hormone deficiencies (MPHD) in 2 cases • Was not realized in 4 cases
RESULTS • MRI performed showed • Pituitary hypoplasia in all patients • Combination with other types of brain damage in 8 cases specified as shown • Disruption of the pituitary stalk in 3 cases(2 with MPHD and 1 without hormonal assessment) • Ectopic posterior pituitary in 3 cases • Chiari I malformation in 1 case • Small size of the corpus callosum with arachnoid cyst in 1 case
RESULTS Fig. 1 :17-year-old boy with growth and pubertal failure:MRI:midsagittal T2 and T1-weighted images, midsagittal and coronal T1-weighted enhancement images show a small anterior pituitary gland (2.8 mm height)(red arrow). Posterior pituitary (yellow arrow)and stalk (green arrow) are normal
RESULTS Fig. 2: 8-year-old girl with growth failure : MRI: coronal and midsagittal T1-weighted images show a small anterior pituitary (2.4 mm height) (yellow arrow) and an ectopic posterior pituitary(orange arrow) seen as an area of high signal intensity in place of the pituitary stalk which is not visible
RESULTS A Fig. 3 : 9-year-old boy with growth failure : MRI: coronal T2-weighted and midsagittal T1-weighted images show a small anterior pituitary (2.5 mm height) (yellow arrow) and Chiari I malformation (orange arrow). Sagittal T2-weighted MR medular image was normal
RESULTS Fig. 4 : 9-year-old boy with hypogonadism and a MPHD in the hormonal assessment : MRI: unenhanced midline sagittal T1 and enhanced coronal T1-weighted images show a small anterior pituitary (3 mm height) (yellow arrow),ectopic posterior pituitary seen as an area of high signal intensity in the midline at the median eminence (orange arrow). The thin stalk is only seen after injection of gadolinium (green arrow)
RESULTS B Fig. 5: 3-year-old boy with facial dysmorphism and growth failure: MRI: midsagittal T1-weighted and coronal T2-weighted images show small anterior pituitary gland (1.9 mm height) (yellow arrow), small size of the corpus callosum (green arrow) and temporal arachnoid cyst (orange arrow)
DISCUSSION • Childhood hypopituitarism may be present at birth or may be acquired • In childhood hypopituitarism, GH is the most commonly underproduced pituitary hormone • The diagnosis of hypopituitarism must integrate clinical data and appropriate hormonal testing • Once the diagnosis of hypopituitarism has been made a head MRI scan must be performed to look for a possible organic or structural basis
DISCUSSION • Laboratory diagnosis is not always easy, the IGHD may be transitory MRI occurs early in the diagnostic strategy, often before laboratory confirmation of the pituitary deficiency • MRI can be used to study the anatomic details of the pituitary-hypothalamic region • The prevalence of morphologic abnormalities in the pituitary gland is greater in patients with combined pituitary hormone deficiency than in those with IGHD
DISCUSSION • Hypopituitarism can be classified in two groups • Congenital Hypopituitarism • Features:hypoglycemia+++ / small penis at birth/ noninfectious form of hepatitis • Causes: birth trauma and/ or asphyxia as part of one of a number of midline anatomical defects / genetic mutation • A congenital basis is strongly suggested by the presence of a transected pituitary stalk on MRI
DISCUSSION • Acquired Hypopituitarism • Causes • Tumor ++: The most common tumor in this region in childhood is craniopharyngioma • Radiation treatment of a cancerous tumor in the head or neck region • Other causes: brain infection (encephalitis and/ or meningitis), hydrocephalus (even without an underlying tumor), vascular abnormalities and major head trauma
DISCUSSION • Abnormalities that can be associated with congenital hypopituitarism include • A small pituitary gland withfilling of the sella with cerebrospinal fluid (empty sella) • Ectopic posterior pituitary gland • Pituitary stalk transection syndrome (lack of pituitary stalk visibility, hypoplasia of the anterior hypophysis, ectopic posterior pituitary gland) • Small optic nerves, hydrocephalus, vascular abnormalities • Midline CNS malformations (optic nerve hypoplasia, Chiari malformation, absence of the septum pellucidum and/ or the corpus callosum)
DISCUSSION • Diagnosis of tumor in the hypothalamic-pituitary area (craniopharyngioma+++) • Lateral skull-ray : erosion of the normal sellar architecture and/ or the presence of suprasellar calcification • MRI show : mixture of solid and cystic components and may contain a ring of calcification around a cystic component
DISCUSSION • Pituitary function was more severely impaired in the patients with pituitary stalk interruptionsyndrome (MPHD) • In contrast, in the patients with isolated pituitary hypoplasia, GH secretion was less severely impaired (IGHD) Correlation between the morphology of the hypothalamic-pituitary axis and endocrine disease severity T1 weighted sequences are the cornerstone of the morphological analysis of the pituitary The injection of gadolinium is more sensitive to visualize the pituitary stalk when it is not seen before injection
DISCUSSION • Treatment of Hypopituitarism • If an underlying cause is discovered on the MRI of the head, such as a tumor and/ or hydrocephalus, appropriate neurosurgical intervention is required • Identified hormone abnormalities require treatment with appropriate hormonal replacement therapies
CONCLUSION • Non-tumor etiology constitutes a major group of childhood hypopituitarism • MRI abnormalities correlated with the severity of growth hormone deficiency • These abnormalities are more prevalent in patients with MPHD than in IGHD • The presence of anterior pituitary hypoplasia should alert the radiologist to the possibility ofassociated cerebral malformations
REFERENCES • J. Hamilton, S. Blaser, D. Daneman. MR Imaging in Idiopathic Growth Hormone Deficiency. AJNR 1998; 19:1609–1615. • P. Dutta, A. Bhansali, P. Singh, R. Rajput, S. Bhadada. Clinico-Radiological Correlation in Childhood Hypopituitarism. Indian Pediatrics 2010; 47: 17. • S. Falcone, J. Sanchez, RM. Quencer. Lack of Normal MR Enhancement of the Pituitary Gland: Findings in Three Siblings with Combined Pituitary Hormone Deficiency. AJNR 1998;19: 287–289. • T. Arrigo, F. De Luca and al. Relationships between neuroradiological and clinical features in apparently idiopathic hypopituitarism. European Journal of Endocrinology 1998; 139: 84–88. • Van der Linden, Hendrik W. van Es. Pituitary Stalk Transection Syndrome with Ectopic Posterior Pituitary Gland. Radiology 2007; 243: 2.