Download

1 / 28
310 likes | 451 Vues
Explore the intricate structure and function of the pancreas, its developmental stages, and the epidemiology of diabetes. Learn about differentiation and regeneration within the pancreas, including the roles of various hormones and signaling pathways.

E N D
Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat theUniversity of Pécs and at the University of Debrecen Identificationnumber: TÁMOP-4.1.2-08/1/A-2009-0011
Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat theUniversity of Pécs and at the University of Debrecen Identification number: TÁMOP-4.1.2-08/1/A-2009-0011 Dr. PéterBalogh and Dr. Péter Engelmann Transdifferentiation and regenerative medicine – Lecture 9 Differentiation and regenerationinthepancreas
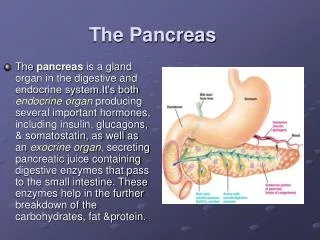
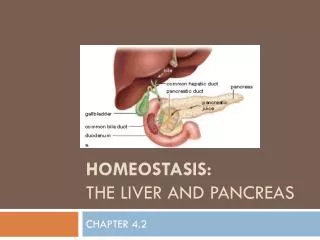
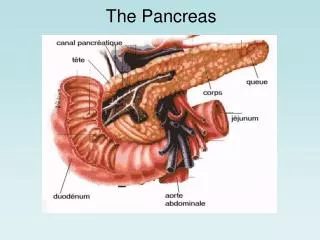
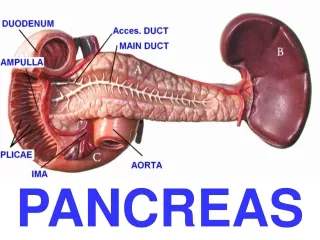
Structure and function of pancreasI • Pancreas is an exocrine and endocrinegland of thedigestivesystem. • The exocrine part represents 95-99% of the totalpancreatic mass. It consists of serous acini ofcellsproducingdigestiveenzymes (lipase, amylase,, phospholipase) as well as pro-enzymes (pepsinogen, elastase, procarboxypeptidase,trypsinogen, deoxyribonuclease, ribonuclease), which are stored in zymogen granules.
Structure and function of pancreasII • The endocrine pancreas is composed of Langerhansislets representing 1-5% of thepancreas. • Adult islets are composed of differentcell types characterized by the production of specific hormones: • Glucagonby a-cells, insulin by b-cells, somatostatin by d-cells andpancreatic polypeptideby PP-cells. A rare fifth endocrine celltype, the e-cell, secreting ghrelin, represents about 1% of theembryonic endocrine pancreas, but disappears after birth. • Insulin and glucagon control blood glucose levels, whereas PP and ghrelinareappetitestimulant(orexigenic) hormones and somatostatin regulates the secretionof insulin, glucagon and PP.
Pancreasphylogeny • First, apperance of pancreashappenedinagnathanfishes (lamprey) representing a collection of b-cellsaroundthebileductinconnectiontotheduodenum. Thisendocrineorgan is composed of 99% b-cells and 1 %somatostatin producing d-cells. • Later, intheancientcartilagousfishes (skates) wecanfoundb-cells are joined by exocrine tissue and a-cells. • Fromsharks, pancreashas also the islet PP-cell compartments.
Specification of the pancreasI • The heart promotes and notochord inhibits liverformation • The notochord promotes, and the heart inhibits pancreasformation • ??? • Pdx1 (pancreatic and duodenalhomeobox 1) expression provides the digestive tube with the ability to form liver or pancreas
Specification of the pancreasII • Notochord activates pancreas development by repressing Shh expression in the endoderm • Shh is expressed throughout the endoderm but repressed where pancreas will develop • FGF2 and activinare secreted in this region by the notochord which are able to downregulate expression of Shh • After establishing the Shh pattern of expression, Pdx1becomes expressed in the pancreatic epithelium.
Embryonicpancreasdevelopment e4.5 e5.5 e6.5 e7.5 e8.5 e9.5 e10.5 e11.5 e12.5 e13.5 e14.5 Mouse 1WD 2WD 3WD 4WD 5WD 6WD Human Oct4 Sox2 Nanog Brachyury T Gsc Gata5 Sox17 Pdx1 Foxa2 Ptf1a Exocrine Hnf4a Sox9 Duct Hhex Hnf1b Duct Mnx1 Onescut1 Duct Ngn3 Nkx6.1 Nkx2.2 Pax6 Neurod1 Pax4 Insm1 MafA
PancreasdevelopmentI • Once pancreatic rudiments are initiated, they begin to form both • Exocrinetissue • Produces amylase anda-fetoprotein • Endocrinetissue • Produces insulin, glucagon and somatostatin • The ratio of exocrine and endocrine cells is regulated by Follistatin – protein secreted by pancreatic mesenchyme (which inhibits BMP4 andactivin) promotes the development of exocrine cells and represses the formation of endocrine cells.
PancreasdevelopmentII • Pax6 is associated with Pdx1. • Mice without Pax6 are deficient of pancreatic hormone production and have malformed islets. • Cells with Pax6andPax4become cells of the islets of Langerhans, and they produce insulin • Those islet cells that down-regulate Pax4 and synthesize only Pax6 become the -cellsthat secrete glucagon
Maintenance of βcellidentity • TGF-bsignalling • MafA • BETA2/NeuroD • Pdx1 • Hedgehogsignalling
Maintenance of αcellidentity • Brn4 • Pax6 • Isl1
Maintenance of exocrineidentity • Pdx1 • Ptf1a • Mist1 • Wnt/-cateninsignaling • Notchsignaling • TGF-signaling
Diabetes epidemiology • Diabetes mellitus is affectingapprox. 200 millionpeopleworldwide. • Therearemore than 37 million diabetic children and adults in NorthAmerica. • In Europe more than 55 millionpeoplesuffersin diabetes.
Main types of diabetes • Type 1 Diabetes • Type 2 Diabetes • LADA (latentautoimmune diabetes of adulthood)
Pathogenesis of type 1 diabetes and β cells • Insulin dependent diabetes mellitus (IDDM) • It can affect children or adults, but most frequently children, that’s why earlier terminology referred it as juvenile diabetes. • Loss of insulin producing beta cells by immune mechanisms. • Hyperglycemia, ketosis • Autoimmune process mediated by the cellular components of immune system. • Autoantibodies (GAD65, IA2, Insulin, etc) • T-cell mediated, Th1/Th2 balance affected, Th1, Tc, macrophage
β cell and autoimmuneprocesses of diabetes Macrophage Cytokines Viruses, endogenousligands? TNF IL-1β INF- INF- and INF-β cell TLR3/4, RIG-I, MDA5, otherreceptors Cytokine receptor signalling T-cell STAT-1, NFB, IRF3, others (?) ↑JunB INF-α and INF-β + - - + MHC class I ER stress Apoptotic signalling Chemokines Cytokines Chemokines Cytokines + Dendriticcell + Presentation of modifiedantigens Celldeath MHC class I Apoptoticβcell T-cell
Process of type I diabetes Trigerringmechanism Normalinsulinsecretion Decreasedinsulinsecretion 100 Normalbloodsugarlevel InsulinC-peptidepresents βcellmass(%) HLA-DR3/4 Autoantibodies, insulitis C-peptide - Immunologicalmalfunctions Metabolicmalfunctions Geneticbackground T1DM Age
Type 2 diabetes • Non-insulindependent diabetes mellitus oradultonset diabetes. • Factorsparctipateinthedisease is life style and geneticbackground. • Insulinresistance • Renalfailure, coronaryarterydisease, retinaldamage
LADA (latentautoimmune diabetes) • 20% of patientsdiagnosedwithtype 2 diabetes actually has LADA. • Low, although sometimes moderate, levels of C-peptide • Autoantibody testing is essential.
Regenerativecapacity of pancreas and βcells • Islettransplantation: Through 1 yearmanypatientsareinsulinindependent, howeverafter5 years of transplantationonly <10% of the recipients remain insulin independent. • β-cell proliferation in adult humans is extremely low, and greatly enlarged islets are rarely found. • Stemcells (embryonic and iPS) could be forcedtogeneratefunctionalβ-cells.
Differentiation of insulin producing β cells from ES cells Fgf11 Cyclopamine Retinoidacid Exendin-4 IGF-1 HGF Activin A Wnt Fgf10 Cyclopamine DAPT Exendin-4 Activin A Human ES cell Oct4 Nanog Sox2 E-cad Mesendoderm Bra Fgf4 Wnt3 N-cad Definitive endoderm Sox17 Cer FoxA2 Cxcr4 Primitive guttube Hnf1b Hnf4a Posterior foregut Hnf6 Pdx1 Hlxb9 Endocrine progenitor Ngn3 Nkx2.2 Pax4 Nkx6.1 Immature endocrine Ins Glu Ghr Som PP Noggin Cyclopamine Retinoidacid Activin A Wnt Keratinocyte growthFactor Activin A In vivo milieu Human ES cell Oct4 Nanog Sox2 E-cad Mesendoderm Bra Fgf4 Wnt3 N-cad Definitive endoderm Sox17 Cer FoxA2 Cxcr4 Primitive guttube Hnf1b Hnf4a Posterior foregut Hnf6 Pdx1 Prox1 Sox9 Pancreatic endoderm/ Endocrine precursors Nkx6.1 Ptf1a Nkx2.2 Ngn3 Endocrine MafA Ins Glu Ghr Som PP
Possible sources of β-cells for cell replacement therapy • β-cells might be generated from existing β-cells through purification and in vitro expansion. • β-cells might be generated via a pancreatic stem cell that could be purified, expanded and differentiated in vitro to generate β-cells. • β-cells might be differentiated in vitro from embryonic stem cells. • β-cells might be directly reprogrammed from patient somatic cells using expression of pancreatic β-cell transcription factors.
β-cellsgenerated from existing β-cells through purification and in vitro expansion • Adultb-cell mass is not static, but fluctuates in response tochanging physiological conditions, such as pregnancy and insulinresistance. • Following partial pancreatectomy,orduringpregnancy, neonatalgrowth, insulinresistance, new b-cells arisefrompre-existingb-cells. • It is possibletoforcebetacelltoproliferatein vitro. • Severalotherstudies suggested alternative origins for b-cells during pancreasregeneration
β-cells generated via a pancreaticstem cell that is purified, expanded and differentiated in vitro to generate β-cells • The ductalcompartmentseemingly represents the site where stem/progenitor cells at leasttransientlyreside. • The progeny of pancreatic ductcells following birth showed thatcarbonycanhydrase II(CAII) expressing cellscan give rise to both endocrine and exocrine cells. • Besides the ductal lining, intra-islet precursor cells as well asacinar cells were suggested to contribute to beta-cell neogenesis.
β-cells differentiated in vitro from embryonic stem cells • Firstattemptswereratherunsuccessfullclaiming ES cellsweredifferentiatedintoinsulinsecretingbetacells, becausethosecellswereinsulinimmune-reactive, but no insulinmRNAorC-peptidewasdetected. It is likely, that ES cellsconsumedinsulinfromtheculturemediacausingthisdiscrepancy. • Recentlyindependentresearchgroupswereabletodifferentiateendocrinecells (includinginsulinproduction) from human ES cellscopyingtheembryonicdevelopment. • Inthesestudies human ES cells can serve as a source of functionalinsulin-producing cells capable of maintaining glucose stably atnormal levels in mice lacking their own beta-cells.
β-cells reprogrammed from somaticcells by expression of pancreatic β-cell transcription factors • Acinar cell culture with the cytokineslikeepidermal growth factor (EGF) and leukemia inhibitory factor (LIF)alongwithexpression of Pdx1, Ngn3, MafAtogeneratefunctionalb-cells. • It is possible to induce the conversion of liver cells (hepatocytes,intra-/extrahepaticbiliary epithelial cells, and gall-bladderepithelium) topancreaticlineages. • A sub-population of intrahepaticbiliary epithelial cells (IHBECs) can be inducedto a b-likephenotype.
Summary • Pancreas is a complex endodermal organ participating in exocrine and endocrine metabolic response. • Great number of human population is suffering in diabetes and have a high risk for developing one of the form of the disease. • In addition to pancreas/islet transplantation other b-cell replacement therapies are considered in clinical research. • One of the promising applications for diabetic patients would be the use of hES or iPS cells to generate functional insulin secreting b- cells.