Download

1 / 24
330 likes | 953 Vues
Factors Influencing Quality lecture 1. Problem Scenario. You want to have an overall view of what can influence the quality of your results concerning a new PCR test on H5N1 which has been set up in your laboratory. Establish the checklist you will use. Organization. Personnel. Equipment.

E N D
Problem Scenario • You want to have an overall view of what can influence the quality of your results concerning a new PCR test on H5N1 which has been set up in your laboratory. Establish the checklist you will use.
Organization Personnel Equipment Process Control (Quality Control & Specimen Management) Information Management Purchasing & Inventory Occurrence Management Assessment Documents & Records Process Improvement Customer Service Facilities & Safety The Quality System
Learning Objectives • At the end of this activity, you will be able to: • Understand the main factors influencing quality of analysis results • Understand the importance of ALL the different factors in the production of reliable results
An Example: HIV Factors influencing quality: • Bad/inadequate sample identification • Contamination (cross-sample contamination, distillated water quality, contaminated micropipettes, reuse of ELISA plates) • Bad incubation of ELISA plates (if needed) • Bad equipment (bad wavelength, etc.) • Bad reagents (expired, bad conservation temperature, low sensibility, inadequacy, etc.) • No or bad quality control (internal/external)
An Example: HIV (continued) Factors influencing quality: • Destruction of the plate’s coating with the micropipette • Misuse of the micropipette (bad tips, bad calibration) • Irregularity of the measurements due to the lack of written techniques • Result transcription mistakes • Result back mistakes (telephone especially) • False positive, false negative
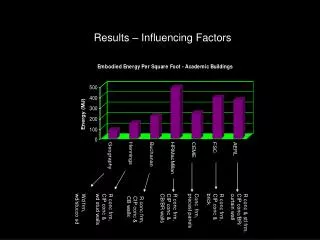
Another Example • Data from JAMA, 1996 • Survey done in the USA • Frequency of laboratory mistakes: 1 %o • 7 % in the analytical step • 93 % in pre/post analytical steps • 45 % of the mistakes are important, with consequences for diagnosis and/or treatment of the disease • Most common mistakes = copying/recopying mistakes
How is quality affected? • The common mistakes: • Analysis prescription • Sampling conditions • Specimen transport and conservation • Training level of technical staff • Reagents and equipment quality • Insufficiency of control procedures • Analytical process • Interpretation of raw results • Transcription and diffusion of the results • Interpretation and use of the results
Analysis Prescription • Bad prescription • Too much: toxoplasmosis IgM for prenatal checking • Not enough: IgG only during acute phase of a disease, pathogen micro-organism without AST, Pneumococcus without penicillin MIC… • Inadequate: normal urine analysis for urethritis, bacteriological analysis after treatment initiation • Incomplete prescription • Suspicion of typhoid fever, stool culture without blood culture or vice versa • No verification of the efficiency of some treatments (stool parasites) • Anarchical self-prescription (low)
Sampling Conditions • Bad identification of the specimen, incomplete or unreadable identification • Inadequate sampling material (contaminated, containing disinfectants, multiple use, bad anticoagulant) • Inadequate timing of samples: • Sampling after ATB treatment begins • Cyclic sampling (filariosis, cortisol) not respected • Sampling outside fever acme (malaria, septicemia) or if hypothermia or if acute phase of the disease (typhoid fever: blood culture before W4) • Long tourniquet time for coagulation tests • Inadequate sample: first drop of urine for standard urine analysis (considered as urethral sample)
Specimen Transport & Conservation • Inadequate conservation delay • Inadequate transportation and conservation temperature • Blood sample badly prepared (slow centrifugation, RBC not separated, frozen without separating RBC) • None or inappropriate transport media (Cary-Blair media for meningitis) • Packaging conditions (biosafety regulations, compatibility with further analysis, addressee contact information) • Addressee absent or not reachable • No follow-up of the specimen by the sender
Training Level of Technical Staff • Insufficient training level: • Sampling • Biosafety • Technical • Analysis management (logbooks, data, reports, conclusions) • Large inter-technician variability (between technicians) • Large intra-technician variability (in one technician) • Lack of continuous training and refreshing • Techniques not standardized, not unified in the country large variability between laboratories • Lack of training for support staff (cleaners, janitors, reagents preparation, etc.) • Inadequation between initial training and current responsibilities
Reagents and Equipment Quality • Usually “least expensive” often “worst quality” • No/little preventive maintenance • No/little meticulous follow-up of the cold chain and how equipment are functioning • No duplication of critical equipment, no possibility to refer the specimen if there are analysis problems • No expiration logbook, use of expired or badly conserved reagents • No check of spectrophotometers and ELISA readers (parasitic light, absorbance, band-width, linearity, etc.) • No periodical calibration of the equipment
Analytical Process • Lack of written technique or containing lots of deletions and changes • Old or imprecise technique (Stokes techniques for AST, Kovacs on urine, AST on pure urine, etc.) • Analysis of the inadequate part of the specimen (sputum for TB, bloody diarrhoea) • Serum pooling! Petri dishes split in two (or even in four), reuse of micropipette tips • Insufficient time devoted to the analysis (20 minutes minimum for malaria and TB)
Insufficiency of Control Procedures • No quality assurance system • No quality supervisor in the laboratory • No national list of registered reagents (or no official use of the list of another country) • No control of culture media, no logbook for the preparation of media and reagents • No positive and negative control for serologies and other analyses • No standardisation of inoculums for AST • No participation in any EQC programme
Interpretation of Raw Results • Total dissociation of the units (chemistry, haematology, bacteriology) problem for global validation • No interpretation of bacterial resistances (no expert system) • Special physiological situations not integrated: • Children/Pregnant women/The elderly • Special pathological situations not integrated: • Renal/liver insufficiency • Dehydration/High temperature • No access to patient history • Lack of critical thinking concerning results • Too much confidence in the automated analyzer
Transcription and Diffusion of Results Reminder: the signing biologist might also be in charge of results transmission • Results transcription mistakes; most common mistake in a laboratory • “Rapid” validation/signature unable to avoid incoherence • Delays in result transmission • Insufficient, incomplete or delayed weekly report to surveillance services
Interpretation and Use of Results • No conclusion or comments on the analysis report • Bad interpretation by the prescriber/clinician • Prescribers lack confidence in laboratory results (Communication? Quality assurance? Other?) • No access to patient history • Incorrect use of the data by surveillance services: • Data integration • Denominator problems
Controllable factors or not? • 2 different types of factors: • Controllable by the laboratory (usually analytical factors) • Non controllable by the laboratory (pre and post analytical factors in general) • Final goal: • Decrease factors controllable by the lab • Communicate with pre and post analytical actors in order to help them control these factors
Summary Cold chain Reagents and consumables Analysis and reports management Organization Sampling Equipment & maintenance Stock managt Training level of the staff IQC, EQCQAM PrescriptionInterpretation Don’t forget Analysis
Summary • Each of the twelve Quality System essentials can be influenced by many factors • This Set of coordinated activities must function as building blocks for quality management.
Problem Scenario • You want to have an overall view of what can influence the quality of your results concerning a new PCR test on H5N1 which has been set up in your laboratory. Establish the checklist you will use.