Download
1 / 167
1.69k likes | 2.13k Vues
Respiratory Failure & Mechanical Ventilation. Dr Sigal Sviri Medical ICU. Contents. Definitions in respiratory failure Oxygen therapy Non-invasive ventilation Indications for intubation Technique Modes of Ventilation (pros and cons) Evaluating & Monitoring ventilated patients

E N D
Respiratory Failure & Mechanical Ventilation Dr Sigal Sviri Medical ICU
Contents • Definitions in respiratory failure • Oxygen therapy • Non-invasive ventilation • Indications for intubation • Technique • Modes of Ventilation (pros and cons) • Evaluating & Monitoring ventilated patients • Ventilation in clinical situations • Weaning from mechanical ventilation
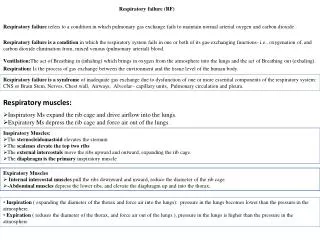
Acute respiratory failure • Acute respiratory failure can be defined as the relatively sudden onset of failure of the respiratory system to carry out its major functions (i.e the adequate delivery of oxygen into and adequate removal of CO2 from the arterial blood) to a degree that cause a threat to life. • A syndrome marked by abnormal physiologic functions that can be caused by a variety of disease processes.
Respiratory Failure • Hypercarbic – type II (reduced ventilation) • Hypoxic type I (reduced gas exchange) • Mixed
Respiratory Failure–Failure to adequately maintain gas exchange:
CNS- reduced drive: Neuromuscular: Musculoskeletal: Airways: Narcotic overdose CVA, ICH, SAH Head trauma Guillain-Barre Myasthenia gravis Spinal cord injury Kyphoscoliosis Flail chest Hemo/pneumothorax Upper airway obstruction/edema Asthma/COPD Ventilation Failure
Alveoli & Capillaries: Pneumonia Pulmonary edema ARDS Interstitial lung dis Pulmonary Embolism Causes of Respiratory Failure
Gas exchange PaO2 = 40 PaCO2 = 46 PaO2 = 150 PCO2 = 0.4 PaO2 = 106 PaCO2 = 40 PaO2 =100 PaCO2 = 40
Definitions Dead space Shunt Compliance Resistance Work of breathing FRC
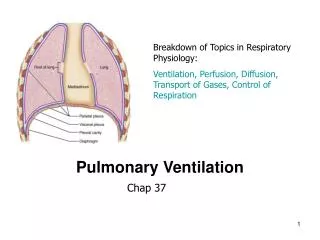
V/Q Ratio • The balance between pulmonary ventilation and capillary blood flow. • Under normal conditions ventilation and perfusion are matched and V/Q=1. • Dead space and shunt are examples of V/Q mismatch.
West zones of the lung (PA > Pa > Pv) (Pa > PA > Pv) (Pa > Pv > PA)
DEAD SPACE (V/Q > 1.0) • Anatomic dead space.The volume of the lung (including the mouth, pharynx, larynx, trachea, bronchi, artificial tubing) which is not involved in gas exchange. • Physiological dead space. • Anatomical dead space plus alveolar dead space. • Alveolar dead space – areas in the lung which are ventilated but not perfused (VQ mismatch)
DEAD SPACE (V/Q>1)יותר אוורור מאשר פרפוזיה • In normal lungs, dead space (Vd) accounts for 20-30% of total ventilation (Vt): Vd/Vt=0.2-0.3 • Increased Vd/Vt causes hypoxemia and hypercapnea. • Hypercapnea is significant when Vd/Vt>0.5. Vd = PaCO2-ETCO2 Vt PaCO2
DEAD SPACE • Lung apices • Emphysema • Positive pressure • Hypovolemia • Shock • Decreased blood flow
DEAD SPACE (V/Q>1) Dead space ventilation increases: • ירידה בתפוקת הלב (heart failure, pulmonary embolism). • הרס מבנה האלבאולים (emphysema) • ניפוח יתר של האלבאולים (positive pressure ventilation)
VQ MISMATCH SHUNT (V/Q<1) Blood does not participate in gas exchange: • True shunt– anatomical shunt between right & left heart • Physiologic shunt:איזורים בריאה שאינם מאווררים • Capillary blood flow to areas of shunt does not participate in gas exchange and does not equilibrate with alveolar gas.
Venous admixture (V/Q<1)פחות אוורור מאשר פרפוזיה • Partial occlusion • Venous admixture –דם לא מחומצן חוזר מהריאות ומתערבב עם דם מחומצן • Because there is some ventilation, increasing FiO2 minimally increases PaO2 (shunt<50%). • שיפור בחמצון עד רמה מסויימת
SHUNT (V/Q=0)מצב אבסולוטי Areas of NO ventilation (fully collapsed lung) Causes : • Occlusion of small airways (asthma) • Alveoli are filled with fluid (pulmonary edema, ARDS, pneumonia) • The alveoli are collapsed (atelectasis) • Blood is unchanged (PaO2 is 40 mmHg) • The hypoxemia CANNOT be corrected by increasing FiO2 • Well ventilated areas cannot compensate because Hb is fully saturated • Adequate oxygenation can only be established by restoring ventilation by recruitment and PEEP
תגובה ל- 100% חמצן • בנוכחות SHUNT אין תיקון מלא של החמצון בתגובה לחמצן אלא אם כן ה- SHUNT קטן • בנוכחות VQ MISMATCHאו ירידה בדיפוזיה, חמצן יתקן באופן מלא או חלקי תלוי בחומרת המצב • בנוכחות היפוונטילציה בלבד, חמצן תמיד יתקן את החמצון אך אינו הטיפול המומלץ!
Pulmonary vasoconstriction • The lung can improve shunt by vasoconstriction of blood vessels in less ventilated areas • May cause pulmonary hypertension
FRC- Functional Residual Capacity • The amount of air remaining in the lungs after a normal quiet expiration (i.e. expiratory reserve volume + residual volume). • If lung volumes are less than FRC, work of breathing is increased.
Recognizing Respiratory Failure • Vital Capacity -The volume of gas that can be forcefully exhaled after maximal inspiratory effort. • Vital Capacity-Reflects patient’s strength and reserve.
Compliance • Distensibility (flexibility) of the lung (& chest wall) during inspiration • The change in volume caused by a change in pressure
COMPLIANCE - The distensibility of the lung Compliance = change in volume change in pressure in mL/cm H20. The normal lung+thorax compliance of an adult is 100 mL/cm H20. When the compliance is low, more pressure will be needed to deliver a given volume of gas to a patient. Peak pressures will be high!
Decreased compliance occurs in: • ARDS, pulmonary edema, pneumonia, atelectasis, pleural effusion, pulmonary fibrosis and interstitial lung disease. • Emphysema is a typical cause of increased lung • compliance.
RESISTANCE- The resistance of the airways to flow • Obstruction/narrowing of the airways and resistance to the flow of air • The flow of air causes high pressure
RESISTANCE- The resistance of the airways to flow Resistance = change in pressure flow in cm H20/L/second The normal value for an adult is around 0.5 - 1.5 cm H20/L/sec Increased airway resistance occurs in: asthma, COPD (acute), emphysema with airway collapse, mucus plugging, endobronchial obstruction either from tumors or foreign bodies, blocked tube.
Restrictive lungs • דלקת ריאות • בצקת ריאות • תמט • מחלת ריאות אינטרסטיציאלית • ARDS • עודף משקל ניכר • חזה אויר
Obstructive lung disease • אסטמה • COPD • אמפיזמה
Work of Breathing • Energy requirements of intercostal muscles and diaphragm. • Increased resistance, reduced compliance, rapid shallow breathing increase work of breathing. • Increased work of breathing may cause lactic acidosis and fatigue. • Mechanical ventilation should decrease the work of breathing.
Recognizing Respiratory Failure Use clinical judgment: • Dyspnea • Tachypnea • Accessory muscles • Shallow breathing • Speech dyspnea • Sweating • Cyanosis • Decreased consciousness
Normal Respiratory Rates in Adult 12 – 20 / min The very important prognostic sign of respiratory failure: RR- tachypnea. A normal rate excludes respiratory dysfunction, but tachypnea > 40 will usually lead to fatigue. Respiratory Rates
Factors Affecting Respiratory Rate: • Fever • Anxiety • Pain • Insufficient oxygen • Insufficient breath • Sleep • Anesthesia/ opiates drugs • Acid-base balance
Recognizing Respiratory Failure • Arterial Blood Gases– Always assess PaO2 in relation to FiO2. Look at trend. • FiO2 may be difficult to assess in non-ventilated patients. • Use Venturi masks, accurate flows.
Oxygenation • PaO2/FiO2 Normal on 21% O2: 100 / 0.21 =~ 500 Shunt on 100% O2 100 / 1.0 = 100 • PaO2/FiO2 < 300 = Acute lung injury
Oxygenation • PaO2/FiO2 • A-a gradient: • Normal < 10 mmHg, or Age/4 +4 • May be normal in hypercapnea (hypoventilation) A-a gradient= PAO2-PaO2 PAO2=FiO2(700-47)-PaCO2/0.8
Oxygenation • A-a gradient: • FiO2 – 0.21, PaCO2 – 40 mmHg, PaO2 – 50 mmHg • What is the A-a Gradient? A-a gradient= PAO2-PaO2 PAO2=FiO2(760-47)-PaCO2/0.8