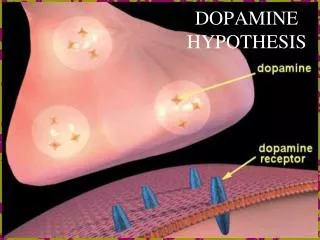
Lecture 4 - Dopamine
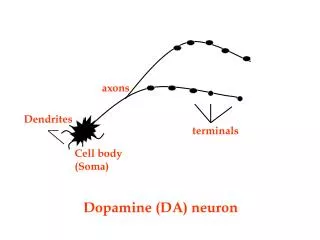
Lecture 4 - Dopamine. Dopamine (DA) systems. 2 major neural pathways: (1) a dorsal (upper) pathway from the substantia nigra (in the brain stem) to the basal ganglia and striatum – also called the nigrostriatal system

Lecture 4 - Dopamine
E N D
Presentation Transcript
Dopamine (DA) systems • 2 major neural pathways: (1) a dorsal (upper) pathway from the substantia nigra (in the brain stem) to the basal ganglia and striatum – also called the nigrostriatal system (2) a ventral (lower) pathway from the ventral tegmental area of the brain stem to the basal forebrain and frontal & prefrontal cortex – also called the mesolimbic system
The dorsal (upper) dopamine system • the nigrostriatal system • is involved in control of movement • neural degeneration causes Parkinson’s disease
Parkinson’s disease • progressive brain disease affecting movement • symptoms – tremor, slowness of movement (bradykinesia), muscle rigidity, stooped posture • about 120,000 people (1 in 500) in the UK have PD • about 10,000 new cases diagnosed each year - 1 in 20 of these under 40 years old • Parkinson’s Disease Society: www.parkinsons.org.uk
Parkinson’s disease • no cure, but dopamine replacement therapy is used to treat symptoms • levodopa (L-dopa) can be converted into dopamine in the brain
Parkinson’s disease • patients also show a distinctive pattern of cognitive impairments affecting ‘executive functions’ (planning, working memory) • and high rates of co-morbid depression (40-50% of patients) • these symptoms are linked to reduced dopaminergic activity in the ventral pathway
Prefrontal cortex (PFC) • the PFC is particularly rich in dopaminergic neurons • frontal executive functions =‘high level’ cognitive abilities involved in planning, monitoring & control of behaviour
Executive functions: Towers of HanoiGet from start position to goal in fewest possible moves (can’t place a larger disc on top of a smaller one)
‘Tower of London’ task (Shallice, 1982) – task difficulty (number of moves) depends on ‘Start’ and ‘Goal’ positions
Tower of London task performance in patients with Parkinson’s disease on & off L-dopa (Lange et al, 1992, Psychopharmacology 107, 394-404) initial thinking time % ‘perfect’ solutions
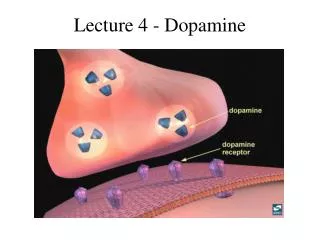
Dopamine & reward • naturally pleasurable and rewarding stimuli (food, sex, etc.) increase DA release in the nucleus accumbensarea of the basal (‘deep’) forebrain • drugs with a high potential for abuse and addiction also increase DA release in this part of the brain
Dopamine & reward • the ventral dopaminergic system normally mediates responses to naturally rewardingstimuli • addictive drugs ‘hijack’ this reward system by inducing DA release, particularly in the nucleus accumbens • some drugs (e.g. amphetamine, cocaine) increase DA by acting directly on dopaminergic neurons within the reward system • others (e.g. alcohol, opiates) increase DA indirectly, via effects on other NT systems
Schizophrenia • schizophrenia = ‘split mind’ • not a ‘split personality’, but a ‘splitting-off’ or disconnection between experience & reality, or thoughts & feelings • 1-2% of people will have at least one ‘psychotic episode’ in their lifetimes • onset is usually between 15 and 35 years old
Dopamine & schizophrenia • ‘Positive’ (or ‘florid’) symptoms - presence of abnormal experiences & behaviour - disordered thought & speech, hallucinations (usually auditory), delusions (often paranoid) - linked to increased DA, especially in basal forebrain areas • ‘Negative’ (or ‘deficit’) symptoms - absence of normal experiences & behaviour - emotional blunting, anhedonia, apathy, social withdrawal, poverty of speech - linked to reduced DA, especially in frontal & prefrontal cortex
The ‘salience hypothesis’ (Kapur 2003) • normally, the occurrence of a motivationally salient (or significant) stimulus or event is signalled by release of DA in the basal forebrain • in psychosis, this process is disrupted so that increased DA coincides with stimuli or events that have nointrinsic significance • this leads to the formation of delusional beliefs to account for subjective experiences of ‘significance’ • similarly, hallucinations are internally generated representations (thoughts, mental images) that have been assigned inappropriate significance
Drugs that reduce DA activity in the brain • antipsychotics: used to treat ‘positive’ symptoms of schizophrenia • chlorpromazine ( = Thorazine), the first anti-psychotic drug (1950) • haloperidol (1957), about 50 times more potent (by weight) than chlorpromazine • originally described as neuroleptics(‘taking hold of nerves’), because reduction in DA produced difficulty in moving • work by blocking dopamine receptors
Potency of antipsychotic effect correlates with a drug’s affinity for dopamine receptors
Mean improvement in symptoms over time in patients taking antipsychotics (combined data from 42 double-blind, placebo- controlled studies; n = 7450) – from Agid et al 2003, Archives of General Psychiatry 60, 1228-1235
Kapur (2004) • neuroleptic drugs are effective in treating the positive symptoms of schizophrenia because, by blocking the actions of DA, they are able to ‘dampen’ the inappropriate experience of salience • but, side-effects can include reduced feelings of salience/motivation for stimuli and experiences in general • referred to as neuroleptic induced dysphoria – feelings of emptiness, apathy, inability to feel pleasure (anhedonia)
Drug “side effects” • neuroleptic antipsychotics • can cause Parkinson-like side-effects • problems withmovement: tremor, rigidity, painful muscle contractions (dystonia) • referred to as ‘motor side-effects’ or ‘extrapyramidal symptoms’ (EPS); linked to reduced DA in the dorsal system • unpleasant subjective reactions to medication: feelings of restlessness (akathisia), emptiness, anhedonia & apathy • referred to as ‘mental side-effects’ or ‘neuroleptic-induced dysphoria’; linked to reduced DA in the ventral system • major reasons for patients stopping medication • but newer ‘atypical’ antipsychotics (clozapine, olanzapine, risperidone) have much reduced side-effects • see Gerlach & Larsen (1999), Tandon & Jibson (2002)
Drugs that increase DA levels in the brain • L-dopa - DA precursor used to treat symptoms of Parkinson’s disease • monoamine oxidase inhibitors (MAOIs) prevent breakdown of DA (& other monoamine NTs – noradrenaline & serotonin) by enzyme MAO • psychostimulants - amphetamine & cocaine
Drug “side effects” • L-dopa • increases levels of DA • can cause schizophrenia-like symptoms in patients • amphetamine & cocaine • increase levels of DA • increase ‘positive’ symptoms in schizophrenia • chronic abuse can cause schizophrenia-like symptoms (paranoia, delusions, hallucinations, stereotyped repetitive & compulsive behaviours) in non-schizophrenics
Amphetamine & Cocaine • these drugs increase levels of both DA & NA • acute effects are similar - reduced fatigue; increased energy, alertness & confidence; increased motor activity & speech • effects of cocaine are more intense and have shorter duration (30-45 mins) than amphetamine • euphoric ‘high’ (due to raised levels of DA in the limbic forebrain - especially nucleus accumbens) means these drugs have a high potential for abuse & dependence
Cocaine blocks reuptake of dopamine, leading to increased concentration in synaptic cleft
Mechanisms of cocaine dependence (Dackis & O’Brien, 2001) • positive reinforcement – acute subjective effects of cocaine are intensely pleasurable • negative reinforcement – unpleasant rebound effects due to dopamine depletion (depressed mood, anhedonia, apathy, lethargy) are reversed by further drug use • classical conditioning– stimuli (including places & people) associated with drug use trigger drug craving
Dopamine (DA) - summary • dorsal (upper) dopaminergic pathway involved in control of movement & is damaged in Parkinson’s disease • ventral (lower) dopaminergic pathway involved in frontal executive functions & pleasure/reward • abnormalities in dopaminergic neurotransmission are implicated in schizophrenia – ‘positive’ symptoms are associated with increased levels of DA, ‘negative’ symptoms with reduced DA • neuroleptics = antipsychotic drugs that reduce dopaminergic activity by blocking DA receptors (but can cause Parkinsonian side-effects & dysphoria) • drugs that increase dopaminergic activity (amphetamine, cocaine) have a high potential for abuse/addiction because of effects in brain ‘reward’ pathways, and can also precipitate psychotic symptoms
Learning outcomes • Understand how the motor, cognitive and mood symptoms of Parkinson’s disease are related to abnormalities in dopaminergic neurotransmitter systems. • Understand how the ‘positive’ and ‘negative’ symptoms of schizophrenia are related to abnormalities in dopaminergic neurotransmission. • Understand the psychopharmacological basis for the therapeutic effects and side-effects of neuroleptic anti-psychotics. • Understand the evidence for the involvement of dopamine in pleasure/reward behaviour. • Understand the role of dopamine in the acute effects of cocaine intoxication and the mechanisms involved in the development of cocaine dependence.
Recommended reading • RA Bressan & JA Crippa (2005) The role of dopamine in reward and pleasure behaviour. Acta Psychiatrica Scandinavica 111, 14-21 • CA Dackis & CP O’Brien (2001) Cocaine dependence. Journal of Substance Abuse Treatment 21, 111-117 • J Gerlach & EB Larsen (1999) Subjective experience and mental side-effects of antipsychotic treatment. Acta Psychiatrica Scandinavica 99 (Suppl. 395), 113-117 • S Kapur (2003) Psychosis as a state of aberrant salience. American Journal of Psychiatry 160, 13-23 • S Kapur (2004) How antipsychotics become anti-‘psychotic’. Trends in Pharmacological Sciences 25, 402-406 • R Tandon & MD Jibson (2002) Extrapyramidal side effects of antipsychotic treatment. Annals of Clinical Psychiatry 14, 123-129