Sickle Cell Anemia (Hemoglobinopathies)
510 likes | 2.06k Vues
Sickle Cell Anemia (Hemoglobinopathies). By: Jessica Hebert, Rob McElroy, Beth McQuinn, Yuway Tsing, Elias Kass, Bill Walter, Amelia Kramer. What are hemolytic anemias?. Decreased life-span of erythrocytes Removal of RBCs may be: Intravascular (within the blood)

Sickle Cell Anemia (Hemoglobinopathies)
E N D
Presentation Transcript
Sickle Cell Anemia (Hemoglobinopathies) By: Jessica Hebert, Rob McElroy, Beth McQuinn, Yuway Tsing, Elias Kass, Bill Walter, Amelia Kramer
What are hemolytic anemias? • Decreased life-span of erythrocytes • Removal of RBCs may be: • Intravascular (within the blood) • Extravascular (within the spleen) • Associated with: • Increased erythropoiesis • Increased hemoglobin catabolism byproducts
Possibilities? • Many types of hemolytic anemias: • G6PD-Deficiency • Hemoglobinopathies • Sickle Cell Disease • Hereditary Spherocytosis • Thalassemias • Immunohemolysis • Others…
Background:Prevalence in Populations • http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Search&db=books&doptcmdl=GenBookHL&term=sickle+cell+prevalence+AND+hstat%5Bbook%5D+AND+340265%5Buid%5D&rid=hstat6.section.17004
Clinical Presentation: Signs and Symptoms http://www.ornl.gov/sci/techresources/Human_Genome/posters/chromosome/sca.shtml
Clinical Presentation • There are a range of Treatments per extremes or per symptoms
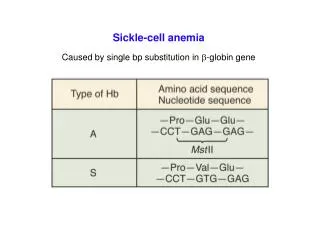
Sickle Cell Anemia A hereditary genetic disorder that results in the production of abnormal hemoglobins
In Sickle Cell, the Beta chain is affected by a point mutation… Source: Robbins
One small point mutation leads to a major problem when HbS is deoxygenated… Deoxyhemoglobin A (HbA) Deoxyhemoglobin S (HbS) http://www.ornl.gov/sci/techresources/Human_Genome/posters/chromosome/hbb.shtml
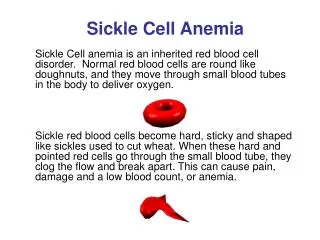
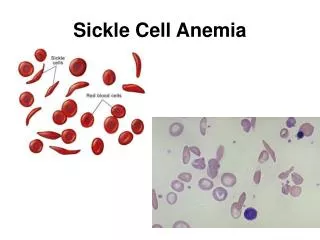
A prolonged environment of low oxygen leads to aggregation and polymerization of hemoglobins into long chains of rod-like fibers, causing the RBC to form the shape of a crescent or sickle. • Donut-shaped • Soft and malleable • Able to pass through small spaces • Lifespan ~120 days • Sickle-shaped • Hard and rod-like • Gets stuck in narrow spaces • Lifespan ~20 days http://www.humanillnesses.com/original/images/hdc_0001_0003_0_img0235.jpg
Sickling of red blood cells leads to: • Vaso-occlusive complications • Severe anemia • Chronic hyperbilirubinemia
Vaso-occlusive complications • Occur in areas with: • Prolonged, low oxygen tension • Decreased pH • Inflammation • Low blood flow Source: Robbins
Severe Anemia and Chronic Hyperbilirubinemia • Young RBCs with HbS can alternate between the sickled and normal formation. • However, sickling causes oxidative damage to the RBCs cell membrane (and to the cells around it). • Eventually, RBCs become irreversibly sickled.
Severe Anemia and Chronic Hyperbilirubinemia • Irreversibly sickled cells end up in the spleen. • Hemolysis occurs at the splenic cords. • Decreased RBCs and increased bilirubin • Infarction and fibrosis causes autosplenectomy. Source: Robbins
12% of males of African descent (A type) 22% of Southeast Asian males (Mahedian type) 50% of Kurdish males (Mediterranean type) Also, a significant prevalence in males of Italian, Greek, Lebanese, Iraqi, and Sephardic heritage (Mediterranean type) G6PD-Deficiency Distribution
G6PD-DeficiencyPresenting Symptoms • Fatigue or muscle weakness • Jaundice or pallor • Dyspnea • Dark urine • Pain (especially abdominal) • Splenomegaly
G6PD-Deficiency – Pathology • Genetic abnormalities (of which there are several varieties) lead to deficient or impaired enzyme function • High levels of oxidants (from foods, drugs, exercise, infections) may damage or denature proteins within the erythrocyte • RBCs may then be subject to intravascular or extravascular hemolysis
G6PD Crisis Precipitation - Beans • Broad beans (favism) • Fava beans, bell beans, fever beans, hava beans, pigeon beans, horse beans, tick beans, silkworm beans, English dwarf beans
G6PD Crisis Precipitation - Oxidizing Drugs • Antimalarials (primaquine, quinine, quinidine) • NSAIDs (aspirin, ibuprofen) • Antibiotics (sulfonamides) • Nitrofurantoin • TCM herbs (rhizoma coptidis, margarita, calculus bovis)
Other oxidants • Henna – primarily infants and pregnant women • Naphthlene (moth balls) – regular exposure
Early Lab Tests – CBC • RBC – Low • Hct – Low • Hb – Low • MCV – Normal to High • MCHC – Low to Normal • MCH – Low to Normal • So…initial CBC is only your starting point
Early Lab Tests – Urinalysis • Hemoglobin • Elevated post-crisis • Bilirubin • Elevated post-crisis • Urobilinogen • Elevated post-crisis • May also see hematuria, proteinuria, LDH • These account for dark color of urine following a crisis, but are also non-specific for any given type of hemolytic anemia
Early Lab Tests - Smear • Often readily seen with initial CBC, or easily ordered alongside • If anemias are suspected, probably best to run a smear in the early stages • G6PD-Deficiency may show: • Heinz bodies • Denatured Hb bound to cell membrane • May damage cell membrane, leading to intravascular hemolysis • “Bite” cells • Spleen removes portion of RBC that had Heinz body, preventing intravascular hemolysis • These aren’t typically present immediately following an acute hemolytic crisis (problem cells have been destroyed)
Other Non-Specific Lab Tests • Reticulocyte count • May be elevated following acute crisis (6-8 weeks) • May be normal in non-crisis situations • May be reduced in aplastic crisis (could go to zero) • Should be considered in conjunction with smear, other data • Serum bilirubin • Present in the unconjugated (prehepatic) form • Elevated after an acute hemolytic crisis • Serum haptoglobin • Binds to Hb in the blood for removal by spleen (preventing Hb from excretion in the urine, which could lead to renal failure) • Decreased (depleted) after an acute hemolytic crisis
Screening for G6PD • Cells from G6PD-deficient subjects can’t convert the oxidized substrate to a reduced state • Different tests use different substrates • Substrates can either be the enzyme’s natural substrate (NADP) or substrates from secondary reactions
Fluorescent Screening Test • G6PD generates NADPH • NADPH fluoresces under long-wave UV light • No G6PD? No fluorescence.
Fluorescent Screening Test • Shortcomings: • False Negative: young red blood cells have more G6PD activity. During an acute hemolytic episode, reticulocytosis results in a bigger population of young red blood cells, so even in G6PD Deficiency, the fluorescence may appear normal. • False Positive: if the patient is anemic, very little fluorescence may be seen because there are very few red blood cells.
Methemoglobin Reduction Test • Sodium nitrite converts Hb (hemoglobin) to Hi (methemoglobin) • Adding methylene blue should stimulate the pentose phosphate pathway, reducing methemoglobin • In G6PD Deficiency, methemoglobin persists
Methemoglobin Reduction Test • Normal blood → clear red color • Deficient blood → brown color • Heterozygotes → intermediate color
Methemoglobin Reduction Test - Takes longer than fluorescence + Extremely inexpensive + Requires only a water bath • Test should be complemented by cytochemical analysis
Cytochemical Analysis • Only way to reliably detect deficiency in heterozygous women • More reliable than assay • Good complement for other tests
Cytochemical Analysis • Treat red cells to convert their oxyhemoglobin (HbO2) to methemoglobin (Hi) • In the presence of G6PD, Hi converts back to HbO2 • Add MTT, which will be reduced by HbO2 to an insoluble form • In G6PD Deficiency: • Hi persists • MTT is not reduced • Ergo, cells are not stained
Cytochemical Analysis • Interpretation: • Normal G6PD activity: majority stained • Hemizygous: majority unstained • Heterozygotes: • Most show mosaicism (40-60% unstained) • Some have only 2-3% unstained (fortunate lyonization)
G6PD Assay • Tracks activity of enzyme by following rate of production of NADPH over time • NADPH has peak of UV light absorption at 340nm • Note potentially misleading results in following table
G6PD Assay Values are examples only (Lewis 10e, p226)
G6PD Assay • Interpretation: • Red cells are likely to lyse from G6PD deficiency if they have less than ~20% of normal enzyme activity • Confounding factors: • With reticulocytosis, the relatively large population of reticulocytes yields a higher enzyme activity, covering up deficiency • Therefore, a low-normal enzyme activity assay during reticulocytosis points towards G6PD deficiency (without deficiency, values would be very high during reticulocytosis) • Re-evaluate after reticulocytosis slows
Choosing Appropriate Tests • More than one test should be used • Are they in the middle of a hemolytic crisis? • Anemia + Reticulocytosis = Misleading results • For females, cytochemical analysis should be used • Normal and deficient control blood should always be used for comparison • Sheep are naturally deficient, bah!