Vasopressor Doses of Epinephrine
Vasopressor Doses of Epinephrine. Push-dose Epinephrine and Epinephrine drips August 1 st , 2019 Protocol #619 – Shock Protocol #641 – Cardiac Arrest (non-traumatic) Protocol #644 – Bradycardia See updates to #640 and #660 in other presentations. Vasopressor Effects of Epinephrine.

Vasopressor Doses of Epinephrine
E N D
Presentation Transcript
Vasopressor Doses of Epinephrine Push-dose Epinephrine and Epinephrine drips August 1st, 2019 Protocol #619 – Shock Protocol #641 – Cardiac Arrest (non-traumatic) Protocol #644 – Bradycardia See updates to #640 and #660 in other presentations
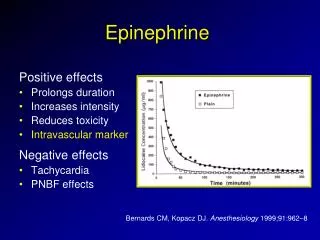
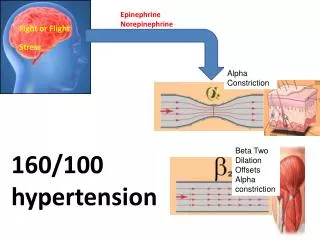
Vasopressor Effects of Epinephrine • Epinephrine is a potent inopressor: • αreceptors – increase peripheral vasoconstriction • Rapidly increases blood pressure by increasing systemic vascular resistance • β1 receptors – increase chronotropy (heart rate) and inotropy (myocardium contraction strength) • Increases cardiac output • Increases heart rate in bradycardias refractory to atropine • β2 receptors - bronchodilation
Vasopressor Types • Push-Dose (PD) epinephrine – started June 1st • Epinephrine Drips – starting August 1st • Dopamine – removing August 1st • Will be completely removed from protocols and stocking requirements • Will remain in the formulary • Paramedic may administer and monitor dopamine drips started by hospital staff
Indications for Use of Pressor Doses of Epinephrine An epinephrine drip OR PD epi are appropriate for hypotensive shock that is NOT caused by hypovolemia: • Hypotension refractory to IV fluids • Potential hypovolemia should be corrected before administering vasopressors • Consider requesting orders to administer vasopressors early if: • Pulmonary edema is present • ROSC with deteriorating vital signs • Critical hypotension, impending cardiovascular collapse • Mean Arterial Pressure (MAP) is <45 mmHg • Consider for bradycardia refractory to other causes • Consider reversible causes of bradycardia
Vasopressor Selection • Push-Dose (PD) epinephrine • Quick and easy method to administer doses of vasopressors to critical patients • 1 mL of PD epi (10 mcg/mL), pushed slowly and repeated as needed • Total dose is similar to that delivered with an epi drip, but is given in short boluses • Administering PD epi may be quicker, and easier in a critical situation then setting up a drip • May be particularly useful in patients rapidly deteriorating towards cardiac arrest • Some patients may only require temporary pressor support and have no need for an ongoing infusion of vasopressors • Epinephrine drips • Starting dose of 10 mcg/mL is similar to dose provided by PD epi • Continuous infusion may allow for finer titration of minimum necessary dose to maintain perfusion • Ideal for patients that need ongoing pressor support following administration of PD epinephrine, particularly during long transports • Base hospital preference may dictate orders for epi drip vs. PD epi
Epinephrine Drip Mixing instructions Epinephrine 1 mcg/mL Date Time • Assemble pre-load of epinephrine 1 mg/10 mL (cardiac epi) • Inject 1 mg of epinephrine into FULL bag of Normal Saline (1 Liter) • Inject through port • LABEL BAG with sticker or cloth tape • “Epinephrine 1 mcg/mL” • Date and time • Bag contains 1 mcg/mL (0.001 mg/mL) • Assemble labelled 1L bag with macro drip tubing • 10 gtts or 15 gtts • Do not administer other medications through the epinephrine drip line Injection Port
Notes - Epinephrine Concentrations • 2016 guidelines from the Institute of Safe Medication Practice • Epinephrine should not be labelled with ratio expressions • Providers should be familiar with the normal expression of epinephrine concentrations • 1mg/mL = 1:1,000 • 1 mg/10 mL (0.1 mg/mL) = 1:10,000 • IM Epi – 1 mg/mL • NEVER to be used IV/IO, for IM injections in anaphylaxis • Cardiac Epi – 1 mg/10 mL = 0.1 mg/mL = 100 mcg/mL • Given IV/IO bolus, typically during cardiac arrest • PD Epi –10 mcg/mL = 0.01 mg/mL • Bolus dose vasopressor • 9 mL of NS with 0.1 mg of epinephrine (1 mL of cardiac epi) • Epi Drip – 1 mcg/mL = 1 mg/L • Vasopressor for infusion • 1 mg of epinephrine in 1000 mL of NS
Epi Dilutions • Ensure any diluted solutions of Epinephrine are labelled clearly and correctly • Take care to make sure dilutions are done correctly • Accidental administration of epinephrine that is too concentrated can result in serious adverse effects including: • Dysrhythmias • Myocardial ischemia • CVA PD Epi 10 mcg/mL Date Time
Dosing Guidelines • Epinephrine Drip: • Up to 10 mcg/min IV/IO infusion. Start infusion at 10 mcg/min • Titrate down to minimum rate to maintain SBP >90 mmHg, or other indicators of response (i.e. heart rate, mental status, skin signs, etc) • Pediatric dose: • 1 mcg/kg (max of 10 mcg/min) IV/IO infusion • Start infusion at recommended dose • Titrate down to maintain age appropriate SBP or other indicators of response • Consider using Metronome (if available) to set drip rate • Push-Dose Epinephrine: • 1 mL IV/IO every 1-3 min • Repeat as needed. No max • Pediatric dose: • 1 mL IV/IO (0.1 mL/kg if <10 kg) every 1-3 min • Repeat as need. No max
Protocol #619 - Shock • Undifferentiated Shock • First-line treatment should focus on IV fluids • Estimated only 34% of patients are given proper fluid challenge prior to administration of vasopressors* • Vasopressors refractory to fluids • Hypovolemic Shock • Treatment should focus on fluid replacement • Septic Shock • First-line treatment – aggressive fluid replacement (consult base as needed) • Vasopressors for critical hypotension or shock refractory to fluids • Cardiogenic Shock • Vasopressors may be considered early * Holden, D. PharmD, et al. Safety Considerations and Guideline-Based Safe Use Recommendations for “Bolus-Dose” Vasopressors in the Emergency Department. Annals of Emergency Medicine, 2017
Protocol #619 - Shock • Physician Consult • Vasopressor doses of epinephrine may be indicated for pediatrics, and other conditions (severe anaphylaxis) • Request Physician Consult as needed • Pediatric considerations • Wide array of differential diagnoses for pediatric shock – most common is hypovolemia • Order requires Physician Consult • During communication failure treatment should focus on fluid boluses * Holden, D. PharmD, et al. Safety Considerations and Guideline-Based Safe Use Recommendations for “Bolus-Dose” Vasopressors in the Emergency Department. Annals of Emergency Medicine, 2017
Protocol #641Cardiac Arrest (atraumatic) ROSC with Persistent Hypotension • Transient hypotension is common in first minutes after ROSC • Fluid bolus is a reasonable first-line treatment • Consider vasopressors for persistent hypotension • Consider early contact for severe hypotension • Consider early contact if vital signs appear to be deteriorating Pediatric Considerations • Indications are the same as adult (age appropriate signs of perfusion) • 1 mcg/kg is appropriate starting dose (max of 10 mcg/min) • Dosing only needs to be adjusted if patient <10 kg • PD epi – 0.1 mL/kg • Epi drip – 1 mcg/kg
Protocol #644Bradycardia • Atropine - First-line treatment for most unstable bradycardias • Consider other reversible causes (i.e. CaCl for hyperkalemia) • Vasopressors – refractory to atropine • Consider early base-contact for orders in unstable high-degree heart blocks • High-degree heart blocks may not respond well to Atropine • 2nd Degree II AVB or Mobitz II • 3rd Degree AVB or Complete Heart Block
Optional references for Push-Dose Epi Detailed information and instructions for PD epi • SLO EMSA Provider Training Page • PD Epi Dilution Demo from Inland Counties EMS Agency End of Presentation Please review: • Tranexamic Acid (TXA) • 2019 General Updates • Pain Management and Fentanyl Questions? Email dbrim@co.slo.ca.us