Download
1 / 62
630 likes | 663 Vues
Unit 21: The Thigh, Hip, Groin, and Pelvis. Anatomy of the Pelvis, Thigh, and Hip. Bony Anatomy. Pelvic Girdle Ilium Iliac crest Anterior superior iliac spine Posterior superior iliac spine Anterior inferior iliac spine. Ischium Ischial tuberosity Hamstring or bursa problems

E N D
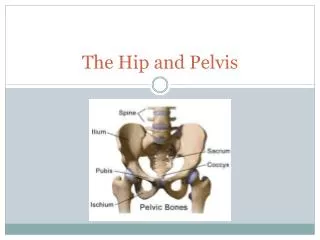
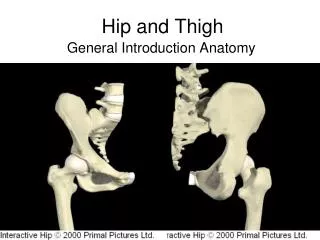
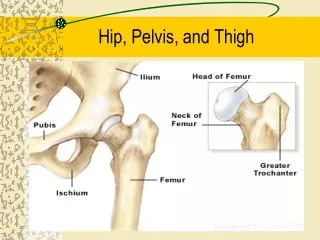
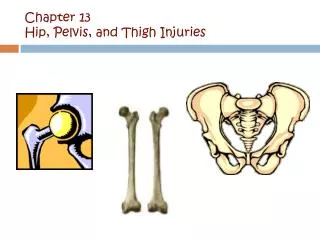
Bony Anatomy • Pelvic Girdle • Ilium • Iliac crest • Anterior superior iliac spine • Posterior superior iliac spine • Anterior inferior iliac spine
Ischium • Ischial tuberosity • Hamstring or bursa problems • Should sit on this area of pelvis • Pubis • Pubic symphysis • Acetabulum
Femur • Head • Neck • Greater trochanter • Lesser trochanter • Shaft • Medial condyle • Lateral condyle
Ligaments - Major source of strength • Ligamentum teres-head of femur • Iliofemoral ligament • Y ligament • Strongest in the body • Prevents hyperextension, external rotation, abduction
Pubofemoral ligament • Prevents abduction • Ischiofemoral ligament • Prevents medial rotation
Bursa • 18 in hip • Ischial bursa • Greater trochanteric bursa • Found at attachment of gluteus maximus and IT band • Iliopsoas
Muscles • Flexors • Iliopsoas • Rectus femoris (quad) • Sartorius • Anterior thigh (quads) • Vastus medialis • Vastus lateralis • Vastus intermedialis
Extensors • Gluteus maximus • Semitendonosis (hamstring) • Semimembranosis (hamstring) • Biceps femoris (hamstring) • Abductors • Gluteus medius • Gluteus minimus • Tensor fascia latae (Iliotibial band)
Adductors • Adductor magnus • Adductor brevis • Adductor longus • Pectineus • Gracilis
External Rotators • Oburator externus • Obturator internus • Quadratus femoris • Piriformis – sciatic nerve goes through it. • Gamellus superior • Gamellus inferior • Gluteus maximus
Internal Rotators • Gluteus minimus • Tensor fascia Latae • Gluteus medius
Assessment of the Thigh • History • Onset (sudden or slow?) • Previous history? • Mechanism of injury? • Pain description, intensity, quality, duration, type and location?
Observation • Postural symmetry? • Size, deformity, swelling, discoloration? • Skin color and texture? • Is athlete in obvious pain? • Is the athlete willing to move the thigh?
Palpation • Soft tissue of the thigh (anterior, posterior, medial, lateral) should be palpated for pain and tenderness • Bony palpation should also be performed to locate areas of pain/discomfort • Utilize palpation to assess body symmetry
Special Tests • Thomas test • Test for hip contractures • Straight Leg Raise • Test for hip extensor tightness • Can also be used to assess low back or SI joint dysfunction Thomas Test
Trendelenburg Test • Gluteus medius • Ober’s/Noble Test • IT Band • Fulcrum
Prevention of Thigh Injuries • Thigh must have maximum strength, endurance, and extensibility to withstand strain • Dynamic stretching programs may aid in muscle preparation for activity • Strengthen programs can also help in preventing injuries
Thigh Injuries • Quadriceps Contusions • Cause of Injury • Constantly exposed to traumatic blows • Signs of Injury • Pain, transitory loss of function, immediate bleeding of affected muscles • Early detection and avoidance of internal bleeding are vital – increases recovery rate and prevents muscle scarring
Care • RICE and NSAID’s • Crutches for more severe cases • Isometric quadriceps contractions should begin as soon as tolerated • Heat, massage and ultrasound to prevent myositisossificans • Padding may be worn for additional protection upon return to play
Myositis Ossificans Traumatica • Cause of Injury • Formation of ectopic bone following repeated blunt trauma • Signs of Injury • X-ray shows calcium deposit 2-6 weeks following injury • Pain, weakness, swelling, decreased ROM • Tissue tension and point tenderness • If condition is recurrent it may indicate problem with blood clotting
Care • Treatment must be conservative • May require surgical removal if too painful and restricts motion (after one year - remove too early and it may come back)
Quadriceps Muscle Strain • Cause of Injury • Sudden stretch-falls on bent knee or experiences sudden contraction • Weakness or over constricted muscle • Signs of Injury • Peripheral tear causes fewer sx than deeper tear • Pain, pt tenderness, spasm, loss of function and little discoloration • Complete tear may leave athlete w/ little disability/discomfort but with some deformity
Care • RICE to control internal bleeding • Determine extent of injury early • Neoprene sleeve may provide some added support
Hamstring Muscle Strains • Cause of Injury • Multiple theories of injury • Hamstring and quad contract together • Change in role from hip extender to knee flexor • Fatigue, posture, leg length discrepancy, lack of flexibility, strength imbalances • Grade 2 - partial tear, identified by sharp snap or tear, severe pain, and loss of function
Signs of Injury • Muscle belly or point of attachment pain • Capillary hemorrhage, pain, loss of function, and possible discoloration • Grade 1 - soreness during movement and point tenderness • Grade 2 – increase pain, swelling, palpable swelling/defect? • Grade 3 - Rupturing of tendinous or muscular tissue, involving major hemorrhage and disability, edema, loss of function, ecchymosis, palpable mass or gap
Care • RICE • Restrict activity until soreness has subsided • Ballistic stretching and explosive sprinting should be avoided initially
Acute Femoral Fractures • Cause of Injury • Generally involves shaft, requires great force • Occurs in middle 1/3 due to structure and point of contact • Signs of Injury • Shock, pain, swelling, deformity • Must be aware of bone displacement and gross deformity • Loss of function
Care • Treat for shock, verify neurovascular status, splint before moving, reduce following X-ray • Secure immediate emergency assistance and medical referral
Femoral Stress Fractures • Cause of Injury • Overuse • Females who are amenorrheic are more vulnerable to stress fx • Signs of Injury • Persistent pain in thigh • X-ray or bone scan • Commonly seen in femoral neck • Management • Analgesics, NSAID’s RICE • ROM and PRE exercises are carried out w/ pain free ROM • Rest, limited weight bearing
Hip, Groin, and Pelvic Injuries • Groin Strain • Cause of Injury • One of the more difficult problems to diagnose • Early part of season due to poor strength and flexibility • Running, jumping, twisting w/ hip external rotation or severe stretch
Signs of Injury • Sudden twinge or tearing during active movement • Produce pain, weakness, and internal hemorrhaging • Care • RICE, NSAID’s and analgesics for 48-72 hours • Determine exact muscle or muscles involved • Rest is critical • Restore normal ROM and strength -- provide support w/ wrap • Refer to physician if severe groin pain is experienced
Sprains of the Hip Joint • Cause of Injury • Result of violent twist due to forceful contact • Force from opponent/object or trunk forced over planted foot in opposite direction • Signs of Injury • Signs of acute injury and inability to circumduct hip • Pain in hip region, w/ hip rotation increasing pain
Care • X-rays or MRI should be performed to rule out fx • RICE, NSAID’s and analgesics • Depending on severity, crutches may be required • ROM and PRE are delayed until hip is pain-free
Dislocated Hip • Cause of Injury • Rarely occurs in sport • Result of traumatic force directed along the long axis of the femur • Signs of Injury • Flexed, adducted and internally rotated hip • Palpation reveals displaced femoral head, posteriorly • Serious pathology • Soft tissue, neurological damage and possible fx
Care • Immediate medical care (blood and nerve supply may be compromised) • Contractures may further complicate reduction • 2 weeks immobilization and crutch use for at least one month