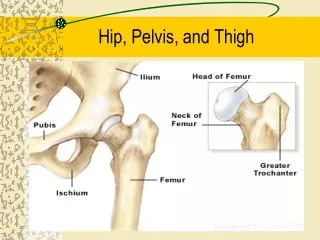
Pelvis and hip
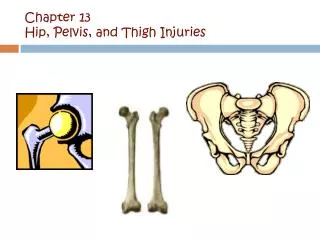
Pelvis and hip. FRACTURES OF THE PELVIS.

Pelvis and hip
E N D
Presentation Transcript
Pelvis and hip FRACTURES OF THE PELVIS
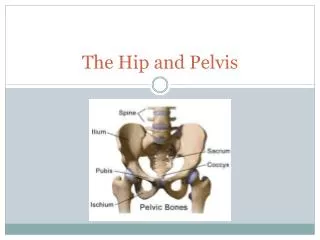
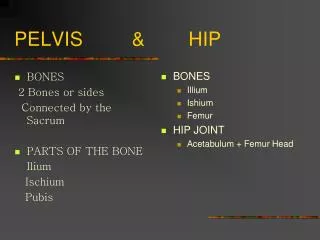
A) Isolated fractures(stable with no disruption of the pelvic ring )[1] Fracture of superior ischio-pubic ramus [2] Fracture of inferior ischio-pubic ramus [3] Fracture entering wall of acetabulum [4] Fracture of wing of ilium[5] Avulsion fractures of anterior inferior iliac spine, anterior superior iliac spine, or ischial tuberosity.
B) Fractures with disruption of the pelvic ring (unstable) [1] Combination of anterior and posterior fractures of the pelvic ring [2] Disruption of pubic symphysis and posterior sacro-iliac joint
DISLOCATIONS AND FRACTURE-DISLOCATIONS OF THE HIP Only three types of dislocation and fracture-dislocation of the hip need be considered: • Posterior dislocation or fracture-dislocation • Anterior dislocation • Central fracture-dislocation. All these injuries are uncommon when compared, for example, with dislocation of the shoulder. Of the three types, the posterior dislocation is the most common.
Diagnosis 1-POSTERIOR DISLOCATION AND FRACTURE-DISLOCATION The femoral head is forced out of the back of the acetabulum by violence applied along the shaft of the femur while the hip is flexed or semi flexed (Fig. 14.4A). The injury often occurs as a result of a motor accident in which the occupant of a car involved in a collision is thrown forwards and strikes the front of the flexed knee against a part of the bodywork. Another common cause is a motor cycle crash.
In about half the cases of posterior dislocation of the hip, the head of the femur carries with it a small or large fragment of bone from the rim of the acetabulum (fracture dislocation; see Fig. 14.6). It should be noted that the sciatic nerve is almost directly in the path of displacement and may easily be damaged.
Clinical features To remember the clinical deformity it is easiest to think of the greater trochanter as being held more or less in its normal position by the attached muscles as if by guy ropes and forming the centre of a new vertical axis about which the femoral head may swing forwards or backwards (Fig. 14.5). Thus in a posterior dislocation the femur and with it the whole lower limb is rotated medially as well as being displaced upwards (Fig. 14,5). There will be true shortening of the limb, perhaps by 2 or 3 cm. Radiographs will confirm the dislocation (Fig. 14.6) and show whether or not there is an associated fracture. Careful examination should always be made for signs of injury to the sciatic nerve.
Treatment The dislocation should be reduced under general anesthesia as soon as possible. Reduction is usually effected without difficulty by pulling longitudinally upon the femur while the hip is flexed to a right angle and rotated laterally. Technique. The patient is placed supine, preferably on the floor or on a low table, and an assistant grasps the pelvis firmly through the iliac crests. The surgeon flexes the hip and knee to a right angle so that the line of the femur points vertically upwards, and then pulls the thigh steadily upwards, at the same time gradually rotating the femur laterally (Fig. 14.4B).
Fig. 14.5 The position of the limb in anterior dislocation and posterior dislocation of the hip. Anterior dislocation: -limb rotated laterally New axis of rotation Posterior dislocation:-limb rotated medially
After the dislocation has been reduced the limb is supported by traction, for 3-6 weeks. Mean while mobilizing exercises for the hip and knee are begun after a few days and are gradually intensified. Complications These are: (1) Injury to the sciatic nerve, (2) Damage to the femoral head, (3) Avascular necrosis of the femoral head, (4) Post-traumatic ossification and (5) Osteoarthritis.
2) ANTERIOR DISLOCATION Anterior dislocation of the hip is much less common than posterior dislocation. Indeed, it is a very uncommon injury. It is caused by forced abduction and lateral rotation of the limb, usually in a violent injury such as a motor accident or aircraft crash. There is not usually an associated fracture of the acetabular margin. Clinically, the limb rests in marked lateral rotation (Fig. 14.5). Treatment Reduction under anesthesia is effected by strong traction upon the limb combined with medial rotation. Thereafter, treatment is the same as for posterior dislocation. Complications There is not the same risk of damage to the sciatic nerve as there is in posterior dislocations, but the femoral nerve and artery may be compressed, and the risk of osteoarthritis from avascular necrosis is the same
3) CENTRAL FRACTURE-DISLOCATION In central fracture—dislocation of the hip the femoral head is driven through the medial wall, or 'floor', of the acetabulum towards the pelvic cavity. It differs from anterior and posterior dislocations in that the capsule remains intact, but there is inevitably a fracture of the acetabulum, usually with much comminution. Central fracture-dislocation is caused by a heavy lateral blow upon the femur, as in a fell from a height onto the side or a crushing injury, or it may be caused by a longitudinal force acting upon the femur (as from a blow upon the flexed knee) while the hip is abducted. The degree of displacement varies withthe severity of the violence
Fig. 14.8 Fracture of the acetabulum with slight medial displacement of the femoral head and acetabular floor. The main part of the weight-bearing surface of the acetabulum is intact. With traction, or failing that by operation, a reasonably smooth acetabular surface may be restored, but there is nevertheless a serious risk that osteoarthritis will develop later.
Treatment Severe shock may demand energetic resuscitation, and the possibility of major internal bleeding should be borne in mind. Treatment of the skeletal injury depends largely upon the degree of comminution and displacement of the acetabular fragments, and upon whether or not it is possible to restore the articular surface to its normal shape. In practice the cases thus fall into two groups: (1) those in which the main part of the weight bearing surface of the acetabulum can be restored to its normal position, congruous with the femoral head; and (2) those in which this is impossible on account of severe comminution of the weight-bearing surface.
W here restoration of the articular surface is possible, non-surgical treatment by skeletal traction through a femoral Steinmann pin will sometimes pull down the displaced fragment of the acetabulum, which should then remain congruent with the femoral head when traction is removed. Traction should, however, be maintained for 4-6 weeks until bony stability has developed. Surgical treatment is indicated when an anterior or posterior fracture dislocation (Fig. 14.9) cannot be reduced by traction.
Fig. 14.9 Severe central fracture-dislocation of the hip (arrows). There is no possibility of restoring a smooth acetabular surface.
Fig. 14.10 CT scans in two planes to show displaced fragments in severe central fracture-dislocation of the hip.
Traction may be continued for symptomatic relief for 2 or 3 days while the fracture is fully evaluated and the most appropriate surgical treatment planned. Ideally patients with these difficult fractures should be transferred to a unit that specializes in their treatment, but this should not be delayed for more than 7-10 days. The incision chosen for treatment depends on the location of the fracture and may require an anterior ilio-inguinal approach, an extended iliofemoral approach, or sometimes a combined anterior and posterior approach. Following open reduction, fixation of the fragments may be achieved by a combination of multiple screws and contoured plates.
In many instances it is necessary to use additional bone grafts to reconstitute skeletal defects resulting from fracture impaction. Surgical complications are frequent, particularly infection and thrombo-embolism and appropriate prophylactic treatment is required. Following surgery, light traction should be continued until wound healing has occurred and weight-bearing is deferred for at least 6 weeks.
It should be borne in mind that many patients with central dislocation of the hip will eventually need total replacement arthroplasty on account of secondary degenerative changes, and one of the objectives of the primary treatment should be to restore the hip sufficiently closely to its normal position to ensure that conditions are favorable for arthroplasty, should it be required.
Complications As in other fractures of the pelvis there may be severe haemorrhage from damage to a major blood vessel, but the common complication is degenerative arthritis from damage to the articular surface of the acetabulum. This may develop early (within a few months) or after a period of years. If the disability from arthritis becomes severe the only effective treatment is by operation. The choice usually lies between arthrodesis and total replacement arthroplasty.
Classification [1] Fracture of the neck of the femur [2] Fracture of the trochanteric region
FRACTURE OF THE NECK OF THE FEMUR Fracture of the neck of the femur is common in persons over the age of 60 years and is one of the so-called 'fatigue fractures . Women are especially at risk, because of a tendency for their bone to become increasingly fragile after the menopause in consequence of generalised osteoporosis. The causative injury is often slight usually a fall or stumble. In most cases the fracture is probably caused by a rotational force. In about 95% of cases, there is marked displacement, the shaft fragment being rotated laterally and displaced upwards, often with comminution of the posterior cortex (Fig. 14.11).
Clinical features A-Displaced fracture. A typical history is that the patient usually an elderly woman tripped and fell, and was unable to get up again unaided. She was subsequently unable to take weight on the injured limb. On examination the most striking feature is the marked lateral rotation of the limb. This is often as much as 90°, so that the patella and the foot point laterally. The limb is shortened by about 2-3 cm. Any movement of the hip causes severe pain. B-Impacted abduction fracture In the exceptional case in which the fracture is impacted, the history and signs are different. The patient may have been able to pick herself up after falling,and she may even have walked a few steps afterwards, perhaps with assistance. Indeed, some patients have remained mobile despite pain, and have not sought medical advice immediately. On examination there is no detectable shortening and no rotational deformity. The patient is able to move the hip through a moderate range without severe pain.
Treatment Displaced fractures and impacted abduction fractures must be considered separately. Displaced fractures. A displaced fracture of the neck of the femur is one of the few fractures that needs rigid immobilization if it is to have any chance of uniting. The alternative treatment, in which the femoral head is excised and replaced by a metal prosthesis, is more commonly used, especially when there is comminution of either fragment, severe displacement, and when the patient is elderly or debilitated.
Fig. 14.12 A) Compression screw-plate (dynamic hip screw) used for some fractures of the femoral neck and for trochanteric fractures. The lag screw(s) gripping the head fragment is drawn into the barrel by tightening the end screw, thus compressing the fragments together. B) Same fracture fixed with parallel long screws.
After operation the patient is nursed free in bed and active hip movements are encouraged. Most surgeons encourage early walking with the aid of crutches or a frame within the first week after the operation on the grounds that in these elderly patients the advantages to the general health of being up and about far outweigh the theoretical advantages to the fracture of rest.
Alternative methods for selected fractures in the elderly. Because of the uncertain results of fixing these fractures by internal devices, especially in the elderly, most surgeons now advise immediate excision of the femoral head and its replacement by a metal prosthesis (replacement arthroplasty, see Fig. 14.17A).
Treatment in children. Femoral neck fracture is uncommon in children, but when it occurs most surgeons advise operative fixation, usually by two or three threaded pins, because bone healing is more reliable and complications fewer. Impacted abduction fractures. It must be emphasized that a diagnosis of impacted abduction fracture should not be made unless both the clinical and radiological criteria of impaction are satisfied (Fig. 14.14). In the absence of such strict criteria, firm impaction of the fracture cannot be assumed, and there is a serious risk that the fragments will fall apart. Despite the feasibility of conservative treatment, there is an increasing trend towards routine internal fixation of impacted abduction fractures, because of a fear that displacement may occur.
Complications Fractures of the neck of the femur are more prone to serious complications than is any other fracture. The important complications are avascular necrosis, nonunion, and late osteoarthritis. All these complications affect fractures with displacement rather than impacted abduction fractures.
Fig. 14.16 Ununited fracture of the neck of the femur with extrusion of the screw that was used for fixation, and redisplacement of the fragments.
Fig. 14.20 Avascular necrosis of a large segment of the femoral head 2 years after fracture of the femoral neck. Although the fracture appears to have united, the ischaemic changes adjacent to the joint margin, with considerable collapse of the bona, are causing osteoarthritis.
Fig. 14.23 Comminuted trochanteric fracture with sub-trochanteric extension. (U Trochanteric fracture after fixation with Gamma nail.
Fig. 14.24 Failure of fixation in a comminuted trochanteric fracture. The screw has cut out from the femoral head.