The Urinary System
440 likes | 457 Vues
Learn about the functions of the kidneys, the anatomy of the urinary system, and the various homeostatic imbalances that can occur.

The Urinary System
E N D
Presentation Transcript
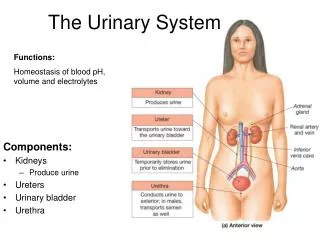
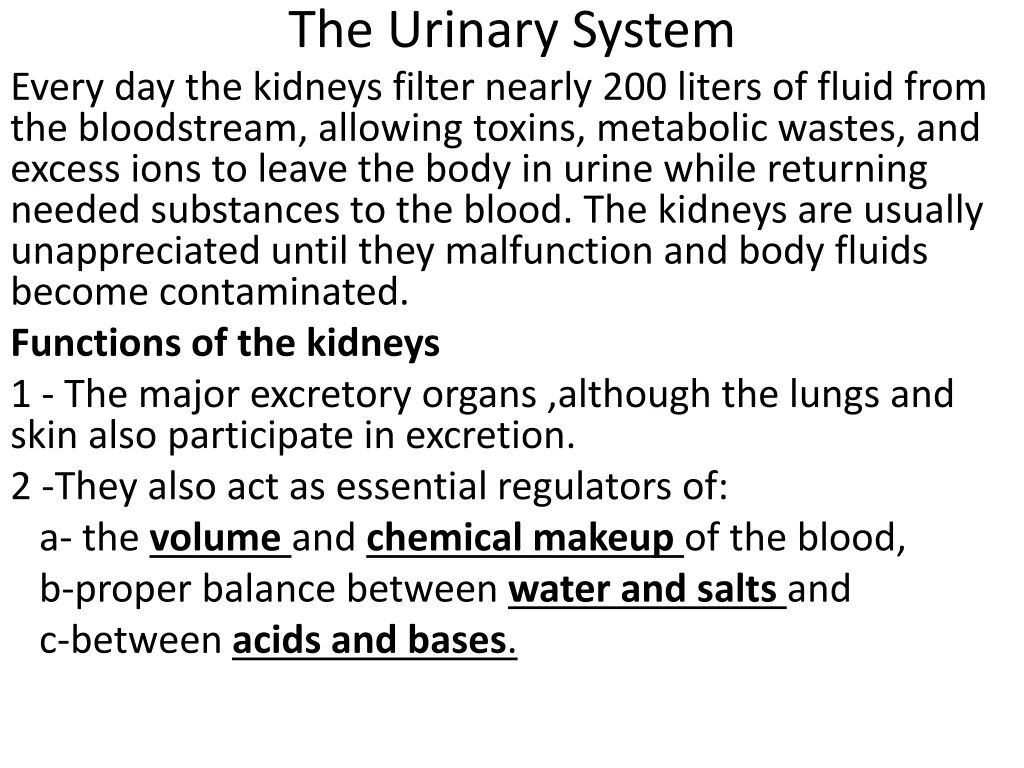
The Urinary System Every day the kidneys filter nearly 200 liters of fluid from the bloodstream, allowing toxins, metabolic wastes, and excess ions to leave the body in urine while returning needed substances to the blood. The kidneys are usually unappreciated until they malfunction and body fluids become contaminated. Functions of the kidneys 1 - The major excretory organs ,although the lungs and skin also participate in excretion. 2 -They also act as essential regulators of: a- the volumeand chemical makeup of the blood, b-proper balance between water and saltsand c-between acids and bases.
Other renal functions include: • Gluconeogenesis during prolonged fasting • Producing the hormonesrenin and erythropoietin -Renin (re′nin; ren = kidney) acts as an enzyme to help regulate blood pressure. -Erythropoietin (ĕ-rith″ro-poi′ĕ-tin) stimulates red blood cell production. • Metabolizing vitamin D to its active form .
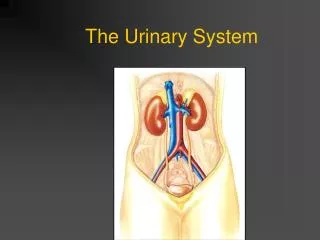
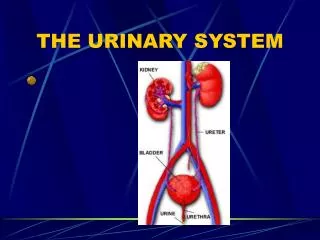
Kidney Anatomy-The bean-shaped kidneys lie in a retroperitoneal position extending approximately from T12 to L3, the kidneys receive some protection from the lower part of the rib cage . -The right kidney is crowded by the liver and lies slightly lower than the left. -An adult’s kidney has a mass of about 150 g and its average dimensions are 12 cm long, 6 cm wide, and 3 cm thick—about the size of a large bar of soap. -The lateral surface is convex. -The medial surface is concave and has a vertical cleft called the renal hilum .
The ureter, renal blood vessels, lymphatics, and nerves all join each kidney at the hilum. • Atop each kidney is the adrenal (or suprarenal) gland. Two layers surround each kidney: 1. The fibrous capsule, a transparent capsule that prevents infections in surrounding regions from spreading to the kidneys. 2. The perirenal fat capsule, a fatty mass that attaches the kidney to the posterior body wall and cushions it against blows
HOMEOSTATIC IMBALANCE The fatty around the kidneys is important in holding the kidneys in their normal body position. If the amount of fatty tissue decreases (as with rapid weight loss), one or both kidneys may drop to a lower position, an event called renal ptosis(to′sis; “a fall”). Renal ptosis may cause a ureter to become kinked, causing hydronephrosis (hi″dro-n ĕ-fro′sis; “water in the kidney”) which can damage the kidney, leading to necrosis (tissue death) and renal failure.
Internal AnatomyA frontal section through a kidney reveals three distinct regions: cortex, medulla, and pelvis. 1-The most superficial region, the renal cortex, is light in color and has a granular appearance. 2 -Deep to the cortex is the darker, reddish-brown renal medulla, which exhibits cone-shaped tissue masses called medullary or renal pyramids. The broad base of each pyramid faces toward the cortex, and its apex, or papilla (“nipple”), points internally.
The pyramids appear striped because they are formed almost entirely of parallel bundles of microscopic urine-collecting tubules and capillaries. • The renal columns, inward extensions of cortical tissue, separate the pyramids. • Each pyramid and its surrounding cortical tissue constitutes one of approximately eight lobes of a kidney.
3-The renal pelvis, a funnel-shaped tube, is continuous with the ureter leaving the hilum. Branching extensions of the pelvis form two or three major calyces (ka′lih-s ĕz; singular: calyx), each of which subdivides to form several minor calyces, cup-shaped areas that enclose the papillae. The calyces collect urine, which drains continuously from the papillae, and empty it into the renal pelvis into the ureter. The walls of the calyces, pelvis, and ureter contain smooth muscle that contracts rhythmically to propel urine along its course by peristalsis.
HOMEOSTATIC IMBALANCE Infections or inflammations that affect the entire kidney are pyelonephritis(pi″ĕ-lo-n ĕ-fri′tis). Kidney infections in females are usually caused by fecal bacteria that spread from the anal region to the urinary tract. Less often they result from bloodborne bacteria (traveling from other infected sites) that lodge and multiply in the kidneys. In severe cases of pyelonephritis, the kidney swells, abscesses form, and the pelvis fills with pus.
Blood and Nerve Supply -The kidneys receive 25% of the total cardiac output per minute. The vascular pathway through a kidney is as follows: renal artery → segmental arteries → interlobar arteries → arcuate arteries → cortical radiate arteries → afferent arterioles → glomeruli → efferent arterioles → peritubular capillary beds → cortical radiate veins → arcuate veins → interlobar veins → renal vein.- The nerve supply of the kidneys is derived from the renal plexus.
NephronsNephrons (nef′ronz) are the structural and functional units of the kidneys. Each kidney contains over 1 million of these tiny units. Each nephron consists of : 1-A glomerulus ,which is a tuft of fenestrated capillaries& 2- A renal tubule. The cup-shaped end of the renal tubule, the glomerular capsule (or Bowman’s capsule) is blind and completely surrounds the glomerulus. This allows large amounts of solute-rich, virtually protein-free fluid (filtrate) to pass from the blood into the glomerular capsule.
The remainder of the renal tubule is about 3 cm long and has three major parts. -the coiled proximal convoluted tubule (PCT), -the loop of Henle -the distal convoluted tubule (DCT) before emptying into a collecting duct. The collecting ducts, each of which receives filtrate from many nephrons, run through the medullary pyramids and give them their striped appearance. As the collecting ducts approach the renal pelvis, they fuse together and deliver urine into the minor calyces via papillae of the pyramids.
NephronCapillary BedsEvery nephron is closely associated with two capillary beds: 1-the glomeruluswhich is specialized for filtration. It differs from all other capillary beds in the body in that it is both fed and drained by arterioles—the afferent arteriole and the efferent arteriole, respectively. Because (1) arterioles are high-resistance vessels and (2) the afferent arteriole has a larger diameter than the efferent: the blood pressure in the glomerulus is extraordinarily high . 2- The peritubular capillaries arise from the efferent arterioles and empty into nearby venules. Most of the filtrate (99%) is reabsorbed by the peritubular capillary beds as they are low-pressure, porous capillaries that readily absorb solutes and water from the tubule cells .
Mechanisms of Urine Formation • Urine formation and the adjustment of blood composition involve three major processes:
Step 1: Glomerular Filtration -The glomeruli function as filters due to high glomerular blood pressure (55 mm Hg), - Usually about 10 mm Hg, the net filtration pressure (NFP) is determined by the difference between forces favoring filtration (glomerular hydrostatic pressure) and forces that oppose it (capsular osmotic pressure) . - About 180 L/day is filtered from the glomeruli into the renal tubules. • Step 2: Tubular Reabsorption Needed substances are removed from the filtrate by the tubule cells and returned to the peritubular capillary blood.
Step Three: Tubular SecretionIs adding substances to the filtrate (from the blood or tubule cells). It is an active process that is important for: • Disposing of certain drugs . • Eliminating of undesirable substances (urea and uric acid). 3. Ridding the body of excess K+. 4. Controlling blood pH. When blood pH drops toward the acidic end of its homeostatic range, the renal tubule cells actively secrete more H+ into the filtrate and retain more HCO3– (a base).
UrinePhysical Characteristics1-Color and Transparency-Freshly voided urine is clear and pale to deep yellow. Its yellow color is due to urochrome (u′ro-krōm), a pigment that results from the body’s destruction of hemoglobin . -The more concentrated the urine, the deeper the yellow color. - An abnormal color such as pink or brown may result from eating certain foods or may be due to the presence in the urine of bile pigments or blood. -Some commonly prescribed drugs and vitamin supplements alter the color of urine. -Cloudy urine may indicate a urinary tract infection.
2-Odor-Fresh urine is slightly aromatic, but if allowed to stand, it develops an ammonia odor as bacteria metabolize its urea solutes. -Some drugs and vegetables alter the usual odor of urine -some diseases. For example, in uncontrolled diabetes mellitus the urine smells fruity because of its acetone content 3- pH-Urine is usually slightly acidic (around pH 6 from about 4.5 to 8.0. 4- Specific GravityThe ratio of the mass of a substance to the mass of an equal volume of distilled water is its specific gravity. The specific gravity of distilled water is 1.0 and that of urine ranges from 1.001 to 1.035, depending on its solute concentration.
Chemical Composition-Water accounts for about 95% of urine volume; the remaining 5% consists of solutes. -The largest component of urine by weight, apart from water, is urea, which is derived from the normal breakdown of amino acids. -Other nitrogenous wastes in urine include uric acid (an end product of nucleic acid metabolism) and creatinine(a metabolite of creatine phosphate, which is found in large amounts in skeletal muscle tissue). -Normal solute constituents of urine, in order of decreasing concentration, are urea, Na+, K+, PO43–, SO42–, creatinine, and uric acid. -Much smaller but highly variable amounts of Ca2+, Mg2+, and HCO3– are also present in urine.
UretersThe ureters are slender tubes that begins at the level of L2 as a continuation of the renal pelvis. From there, it descends behind the peritoneum and runs obliquely through the posterior bladder wall. This arrangement prevents backflow of urine. The transitional epithelium of its lining mucosa is continuous with that of the kidney pelvis superiorly and the bladder. Incoming urine distends the ureter and stimulates its muscularis to contract, propelling urine into the bladder. (Urine does not reach the bladder through gravity alone).
HOMEOSTATIC IMBALANCE -Calcium, magnesium, or uric acid salts in urine may precipitate in the renal pelvis, forming renal calculi or kidney stones. Most calculi are under 5 mm in diameter and pass through the urinary tract without causing problems. However, larger calculi can obstruct a ureter and block urine drainage. -Predisposing conditions are frequent bacterial infections, urine retention, high blood levels of calcium, and alkaline urine. Surgical removal of calculi has been almost entirely replaced by shock wave lithotripsy, a noninvasive procedure that uses ultrasonic shock waves to shatter the calculi.
Urinary BladderThe urinary bladder is a smooth, collapsible, muscular sac that stores urine temporarily. It is located retroperitoneally on the pelvic floor just posterior to the pubic symphysis. The prostate (part of the male reproductive system) surrounds the bladder neck inferiorly where it empties into the urethra. In females, the bladder is anterior to the vagina and uterus. The interior of the bladder has openings for both ureters and the urethra .The smooth, triangular region of the bladder base outlined by these three openings is the trigone (tri′gōn; trigon = triangle), important clinically because infections tend to persist in this region.
The bladder has mucosa containing transitional epithelium .It`s muscular layer is called the detrusormuscle. When empty, its walls are thick and thrown into folds (rugae). • A moderately full bladder holds approximately 500 ml of urine. • When tense with urine, it can be palpated well above the pubic symphysis. The maximum capacity of the bladder is 800–1000 ml and when it is overdistended, it may burst.
The Pelvis Figure 8–8
UrethraThe urethra is a thin-walled muscular tube that drains urine from the bladder and conveys it out of the body. At the bladder-urethra junction has: - The involuntaryinternal sphincter that keeps the urethra closed .This sphincter is unusual in that contraction opens it and relaxation closes it. -The voluntary externalurethral sphincter which is formed of skeletal muscle and is voluntarily controlled. The levatorani muscle of the pelvic floor also serves as a voluntary constrictor of the urethra .
In females the urethra is only 3–4 cm long and straight while in males the urethra is approximately 20 cm long , curved and has three regions: - The prostatic urethra, about 2.5 cm (1 inch) long, runs within the prostate. -The membranous urethra, which runs through the urogenital diaphragm, extends about 2 cm from the prostate to the beginning of the penis. -The spongy urethra, about 15 cm long, passes through the penis and opens at its tip via the external urethral orifice.
- The male urethra has a double function: It carries semen as well as urine out of the body. -The male urethra opens away from anus while the female’s external orifice is close to the anal opening. • HOMEOSTATIC IMBALANCE -Overall, 40% of all women get urinary tract infections. -The urethral mucosa is continuous with that of the rest of the urinary tract, and an inflammation of the urethra (urethritis) can ascend the tract to cause bladder inflammation (cystitis) or even renal inflammations (pyelitis or pyelonephritis).
MicturitionMicturitionalso called urination or voiding, is the act of emptying the bladder. Stretching of the bladder wall by accumulating urine initiates the micturitionreflexthat cause the detrusor muscle to contract and the internal urethral sphincter to open. Because the external sphincter is voluntarily controlled, micturition can usually be delayed temporarily.
HOMEOSTATIC IMBALANCE -Incontinenceoccurs when we are unable to voluntry control the external urethral sphincter. It isnormal in children 2 years old or younger. -Urinary retention, the bladder is unable to expel its contained urine. -Urinary retention is normal after general anesthesia . -Urinary retention in men often reflects hypertrophy of the prostate, which narrows the urethra, making it difficult to void.
Fluid and Electrolyte BalanceWater accounts for 45–75% of body weight, depending on age, sex, and amount of body fat.Fluid Compartments • About two-thirds (25 L) of body water is found within cells ,intracellular fluid (ICF) compartment; the extracellular fluid (ECF) compartment (15 L) is about one-third. The ECF includes plasma (3 L)and interstitial fluid(12 L).
Fluid Movement Among Compartments Fluid exchanges between compartments are regulated by osmotic and hydrostatic pressures: (a) Filtrate is forced out of the capillaries by hydrostatic pressure and pulled back in by colloid osmotic pressure. (b) Water moves freely between the ECF and the ICF by osmosis, but solute movements are restricted by size, charge, and dependence on transport proteins.
Water Balance -Sources of body water are ingested foods and fluids and metabolic water. - Water leaves the body via the lungs, skin, gastrointestinal tract, and kidneys.Regulation of Water Intake Increased plasma osmolality triggers the thirst mechanism, mediated by hypothalamic osmoreceptors. Regulation of Water Output includes insensible water losses from the lungs, the skin, in feces, and about 500 ml of urine output daily.-Thevolume of urinary output depends on water intake and the influence of antidiuretichormone and aldosteroneon the renal tubules.
Acid-Base Balance - The homeostatic pH range of arterial blood is 7.35 to 7.45. A higher pH represents alkalosis; a lower pH reflects acidosis.Acid-base balance is achieved by: 1-Chemical Buffer Systems that include the bicarbonate, phosphate, and protein buffer systems 2-Respiratory regulation -Acidosis activates the respiratory center to increase respiratory rate and depth, which eliminates more CO2 and causes blood pH to rise. -Alkalosis depresses the respiratory center, resulting in CO2 retention and a fall in blood pH.
3- Renal Regulation The kidneys provide the major long-term mechanism for controlling acid-base balance by maintaining stable HCO3– levels in the ECF.-To counteract acidosis, H+ is excreted in urine -To counteract alkalosis, bicarbonate ion is secreted into the filtrate and H+ is reabsorbed. Abnormalities of Acid-Base Balance - Classification of acid-base imbalances is based on the cause : - Respiratory acidosis results from carbon dioxide retention. - Respiratory alkalosis occurs when carbon dioxide is eliminated faster than it is produced.
- Metabolic acidosis occurs when fixed acids (lactic acid, ketone bodies, and others) accumulate in the blood or when bicarbonate is lost from the body. - Metabolic alkalosis occurs when bicarbonate levels are excessive. - Extremes of pH for life are 7.0 and 7.8.Compensations occur when the respiratory system or kidneys act to reverse acid-base imbalances. -Respiratory compensations involve changes in respiratory rate and depth. -Renal compensations modify blood levels of HCO3–.