Download
1 / 43
490 likes | 1k Vues
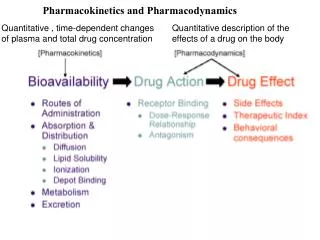
Pharmacokinetics and Pharmacodynamics. Quantitative , time-dependent changes of plasma and total drug concentration. Quantitative description of the effects of a drug on the body. Pharmacokinetics and Pharmacodynamics.

E N D
Pharmacokinetics and Pharmacodynamics Quantitative , time-dependent changes of plasma and total drug concentration Quantitative description of the effects of a drug on the body
Pharmacokinetics and Pharmacodynamics Pharmacodynamicsis the study of how drugs interact with a molecular target, i.e; effect of the drug on the body. Pharmacokineticsis the study of how a drug reaches its target in the body and how it is affected on that journey, i.e; effect of the body on the drug. Pharmacokinetics is the study of how is the drug absorbed, distributed, metabolized and excreted in the body 2
Efficacy is the maximal response a drug can produce Potency is a measure of the dose needed to produce a response and is expressed as the dose required to achieve 50% of the desired therapeutic effect.
TI= TD50 ED50
e.g. Heparin TI < 2 measure PTT Aspirin TI 1000
Clinical effects of drug action have the dualism, The aim of drug therapy is to cure or suppress disease, called therapeutic action, but also bring about some harmful effects, named untoward or adverse reaction. Therapeutic Effect It implied the effects that conform the goal of therapy, including etiological treatment and symptomatic treatment. 1.etiological treatment implies primary therapy (e.g. in bacterial and parasitic infections), when the disease is eliminated and the drug is withdrawn; or auxiliary therapy, also called supplement therapy or replacement therapy. 2.symptomatic treatment means suppression of diseases or symptoms is used continuously or intermittently to maintain health without attaining cure (as in hypertension, diabetes, epilepsy, asthma) or to control symptoms (such as pain and cough) whilst awaiting recovery from the causative disease. Generally, etiological treatment is more important than symptomatic treatment. However, symptomatic treatment is not necessarily trivial in emergency rescue, such as heart failure, shock, epilepsy, asthma, etc.
Adverse Reaction (Untoward) The term adverse reaction is defined as unwanted, seriously unpleasant, or even harmful effects. 1. Side effectsis to be the undesired effects unrelated to therapeutic aim and occurring at doses intended for therapeutic effect. ①It is often slight, recoverable functional alteration of the body. ②Some of side effects may make a quick recovery without withdrawal of the drug, but others dose not disappear until withdrawal of the drug. ③The pharmacological basis of side effect is lower selectivity ④Side effects vary with different therapeutic goals. For example, atropine is used as an antisecretory agent to block secretions in the upper and lower respiratory tracts prior to surgery . ⑤Usually drug in combination is the best way to prevent from side effects.
2. Toxic reaction is the adverse reactions that occur frequently due to overdose or longterm use. ①Any drug in overdose could induce toxicity, which implied a direct action.The toxic reactions vary with different drugs, but much of the serious drug toxicity in clinical practice represents a direct pharmacological extension of the therapeutic action of the drug, thus they are predictable. ②The severity of a toxicity is deteriorated with dose increase, so we cannot rise the therapeutic effect by increasing doses of drug, which is very dangerous. ③Toxicity can not automatically disappear because it often damages the function or the morphology of organs, even inducing teratogenicity, carcinogenicity and mutagenicity. Toxicities include the acute toxicity, subacute toxicity and chronic toxicity 3. Residual effect implies the biological responses induced by residual drug below effective concentration after cessation of administration, including a short period, long term and permanent. 4. Withdrawal reaction implies a worsening of original diseases occurred after suddenly cessation of administration, also called the rebound reaction.
Agonists and antagonists Two states: closed or open
An antagonist is a molecule that inhibits the action of an agonist but has no effect in the absence of an agonist e.g. protamine binds heparin
e.g. Pravastatin inhibits HMG CoA Reductase, which is the rate limiting enzyme in cholesterol synthesis e.g. aspirin is a noncompetitive antagonist. It acetylates cyclooxygenase -reduced efficacy -same potency
Raloxifene = SERM (selective estrogen receptor antagonist Bone is a Partial agonist Breast is an antagonist Inverse agonist decrease inherent activity of receptor e.g BCR-Abl Spare receptors : a maximal response is achieved with < 100% occupancy e.g. GPCRs where one G protein can stimulate second messenger formation.
Thiopental and diazepam in fat Heparin to plasma proteins
First-Pass Metabolism can occur with orally administered drugs
Bioavailability = Quantity of drug reaching the circulation Quantity of drug administered 1. First-Pass hepatic metabolism e.g P450 enzymes in liver transform drug Solubility: extremely hydrophilic and hydrophobic drugs are poorly absorbed Instability: penicillin G is unstable at low pH, insulin is digested
Route Advantages Disadvantages Enteral Simple, inexpensive Drug exposed to GI and e.g. aspirin painless first-pass metabolism, slow delivery Parenteral Rapid delivery Irreversible, infection e.g. morphine no first-pass metabolism pain, skilled personnel high bioavailability Mucous Rapid delivery, simple Few drugs Beclomethasone No first-pass metabolism (Sublingual,nasal, rectal) Direct delivery (lungs) Transdermal Simple, prolonged admin. lipophilic drug Nicotine No First-pass slow delivery Routes of Drug Administration
Parenteral Drug Administration Advantages Disadvantages Subcutaneous slow onset, oil based slow onset, small vol. Xylocaine Intramuscular Intermediate onset, oil-based hemorrhage, pain Haloperidol Intravenous Rapid onset, controlled peak-related toxicity morphine delivery Intrathecal Bypasses BBB Infection, skilled methotrexate personnel
pKa= pH + log [HA] [A-] 3=log [HA] [A-] 1,000= [HA] [A-]
Most drugs are rapidly distributed from the systemic circulation to other compartments e.g. interstitium and adipose tissue See Table 3-3 e.g. diazepam (valium) Half-life: time for drug conc to decrease to half its original value First-order kinetics: the amount of drug metabolized or excreted is proportional to the conc in the systemic circulation i.e the fraction eliminated remains the same.
e.g. Warfarin And fluoxetine (Prozac)
45% whites and Blacks are slow acetylators; 90% Asians "Fast acetylators"
Prodrugs: Tamoxifen, codeine See table 4-3 Fluoxetine; CCB, grapefruit Anti-HIV
Question: Which of the following statements is correct? The greater the number of receptors occupied by a drug, the greater the potency. Drugs with high potency have a high EC50. Drugs with high potency have a drug DR curve that lies to the right of a less potent drug The presence of a competitive antagonist shifts the agonist DR curve to the right and decreases the potency The greater the drugs potency, the higher its drug receptor dissociation constant, Kd. Ans. D The potency is the conc at which the drug elicits 50% max response. Very potent drugs have a low EC50. In 4, the binding of a competitive antagonist alters the equilbrium binding of the agonist. The greater a drugs potency the lower its Kd.
Question: What properties of certain drugs, such as aspirin, allow them to be taken without monitoring plasma drug levels, whereas heparin requires monitoring. Whereas aspirin is taken orally, heparin is administered parenterally Aspirin is available without prescription and can be taken safely Whereas aspirin events are irreversible, which does not need monitoring, the reversible effect of heparin must be monitored. 4. Whereas aspirin causes a graded DR relationship, heparin causes a Quantal DR relationship that must be monitored. Whereas aspirin has a larger therapeutic index, heparin has a small TI. Ans. E. Heparin has a TI <2 I.e it can cause toxicity and bleeding at less than twice the therapeutic dose.
Your patient, Mr. S, is a 65-year old man that you are monitoring for elevated BP. His BP is 145/105 mm Hg this morning. You decide to to give a diuretic, thiazide and a beta-receptor blocker as an anti-hypertensive therapy. As you decide between atenolol and propranolol you remember that thiazide is 95% bound to albumin plasma protein. Atenolol Propranolol Plasma protein binding 5% 95% Urinary excretion 85% 1% HOW DOES THE DIFFERENTIAL BINDING DETERMINE WHICH DRUG TO USE? Atenolol is less bound and so has less ability to reach the receptor Atenolol is less bound and so is less likely to interfere with plasma binding of thiazide Propranolol is highly bound, so it is less likely to displace thiazide Propranolol is highly bound, so it is more likely to compete with thiazide Propranolol is highly bound, so it will require a lower dose to achieve effect similar to atenolol Ans. B. Atenolol is less likely to displace thiazide. Propranolol is expected to displace thiazide. Drugs that are bound to plasma proteins may require a higher dose to achieve a therapeutic effect.
Ms. B is a 32-year old woman who complains of a sore throat. Physical exam reveals creamy white lesions on the tongue that is identified as oral thrush, a fungal infection. Her history includes sexual activity with multiple partners, inconsistent use of condoms. She is diagnosed wth an HIV-1 infection, confirmed by PCR. She is started on an anti-HIV regimen that includes the protease inhibitor sequinavir. Despite this treatment she presents several months later with a persistent cough that turns out to be TB. What factors should the physician consider when deciding a course of treatment with the anti-TB drug, Rifampin. If oral thrush is present it will prevent GI absorption of oral contraceptives The MDR1 transporter will block GI absorption of anti-TB agents in HIV patients The metabolism of sequinavir will be enhanced by anti-TB drugs The metabolism will be enhanced by drinking grapefruit juice Renal excretion of anti-TB drugs is prevented by sequinivir Ans C. Rifampin induces P450 3A4 and so will enhance metabolism of sequiniavir. The MDR1 actively transports drugs back into the intestine. Grapefruit juice contains psoralen that inhibit P450 and so may reduce metabolism.
CASE: Mr W is a 66 year old technology consultant. His only medical Problem is chronic atrial fibrillation, and his only medication is WARFARIN. He flies to Turkey where he eats shish kebabs. The next day he develops foul smelling diarrhea and his physician precribes a 7 day course of trimethoprim-sulfamethoxazole. He feels well for 2 days and goes on another dinner where much alcohol was consumed. Upon leaving the restaurant he falls and the next day he has a swollen knee. Upon examination and lab studies show a elevated International Normalized Ratio, which is a standardized measure of Prothrombin time- a surrogate marker of for warfarin levels. The physician advises Mr W that his warfarin level is in the supra- Therapeutic (toxic) range and is likely the result of an adverse drug- Drug interaction between warfarin and the antibiotics (and the recent Alcohol!).
What was the cause of Mr. W's supratherapeutic Warfarin level? Trimethoprim inhibited the hepatic metabolism and clearance Trimethoprim enhanced growth of GI bacteria that normally Degrade warfarin C. Trimethoprim has an anticoagulant adverse effect Trimethoprim competed with warfarin for binding to its receptor E. Trimethoprim prevented the renal secretion of warfarin Ans. A. Trimethoprim inhibited the hepatic metabolism of warfarin. In addition the ethanol also inhibited metabolism.