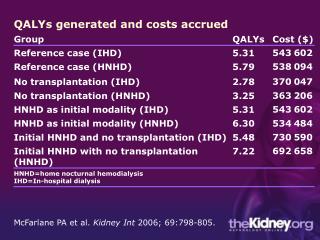
The QALYs debate
The QALYs debate. Prof. dr. Jan J.V. Busschbach, Ph.D. Erasmus MC Institute for Medical Psychology and Psychotherapy. Health Economics. Comparing different allocations Should we spent our money on Wheel chairs Screening for cancer Comparing costs Comparing outcome

The QALYs debate
E N D
Presentation Transcript
The QALYs debate • Prof. dr. Jan J.V. Busschbach, Ph.D. • Erasmus MC • Institute for Medical Psychology and Psychotherapy
Health Economics • Comparing different allocations • Should we spent our money on • Wheel chairs • Screening for cancer • Comparing costs • Comparing outcome • Outcomes must be comparable • Make a generic outcome measure 2
Outcomes in health economics • Specific outcome are incompatible • Allow only for comparisons within the specific field • Clinical successes: successful operation, total cure • Clinical failures: “events” • “Hart failure” versus “second psychosis” • Generic outcome are compatible • Allow for comparisons between fields • Life years • Quality of life • Most generic outcome • Quality adjusted life year (QALY) 3
Quality Adjusted Life Years (QALY) 1.00 X 0.00 0.5 x 80 = 40 QALYs 80 40 Life years • Example • Blindness • Time trade-off value is 0.5 • Life span = 80 years • 0.5 x 80 = 40 QALYs 4
Time Trade-Off • TTO • Wheelchair • With a life expectancy: 50 years • How many years would you trade-off for a cure? • Max. trade-off is 10 years • QALY(wheel) = QALY(healthy) • Y * V(wheel) = Y * V(healthy) • 50 V(wheel) = 40 * 1 • V(wheel) = .8
Standard Gamble • SG • Wheelchair • Life expectancy is not important here • How much are risk on death are you prepared to take for a cure? • Max. risk is 20% • wheels = (100%-20%) life on feet • V(Wheels) = 80% or .8
Which health care program is the most cost-effective? A new wheelchair for elderly (iBOT) Special post natal care 9
www.ibotnow.com Dean Kamen Segway 10
Which health care program is the most cost-effective? • A new wheelchair for elderly (iBOT) • Increases quality of life = 0.1 • 10 years benefit • Extra costs: $ 4,000 per life year • QALY = Y x V(Q) = 10 x 0.1 = 1 QALY • Costs are 10 x $4,000 = $30,000 • Cost/QALY = 40,000/QALY • Special post natal care • Quality of life = 0.8 • 35 year • Costs are $250,000 • QALY = 35 x 0.8 = 28 QALY • Cost/QALY = 8,929/QALY 11
Milton Weinstein In the face of uncertainty … and fear The decision will be made, if not actively then by default
QALY = Utility: Welfare theory • QALY can be see as the ‘value of health’ • The value of a good or service: “utility” • Also called “nut” (Dutch) • Welfare theory: maximize utility • Maximize QALY • Do we want to maximize QALY? • Doubtful…
Is the utility scale valid? 1.0 Utility of Health B 0.0 B C A 16
Critique • We do not maximize QALY • But nevertheless we want to maximize utility • By (economic) definition.. • That means: • QALYs measured utility in an invalid way • Life years is not the problem, thus… • It must be the validity of quality of life assessment… 17
…it must be that QALYs are invalid We don’t like the results…
In the past, much criticism Cohen CB. Quality of life and the analogy with the Nazis. Journal of Medicine and Philosophy 8: 113-35, 1983.
Criticism remains ….the strictly fascist essence of those QALYs (so-called Quality-Adjusted Life Years)…
Burden as criteria Pronk & Bonsel, Eur J Health Econom 2004, 5: 274-277 21
?? persons 1 year free from disease Q 100 persons additionally 1 healthy year Person Trade-Off • Values between patients • Not ‘within’ a patient like SG, TTO and VAS • Better equipped for QALY? • V(Q) = 1 - (A / B) • For instance: • V(Q) = 1 - (100/300) • V(Q) = 1 - 0.33 • V(Q) = 0.67
PTO and it’s psychometrics • Paul Kind: • If we look at TTO and PTO... • we see that one of them is wrong • If we look at PTO alone... • We still see that one of them is wrong... PTO is not a quick fix
Falsification even with life years B B C A Life Years 25
Utility? 1.0 Utility of Health B 0.0 B C A 26
Utility Utility Total benefit Including distribution Also called “Nut” (Dutch) Quality of life might be part of total benefit QALYs do not include distribution But it is said that ‘Standard Gamble’ measures utilities! Van N-M utilities by definition utility But in SG only “health for your self” Does not include distribution
Costs/QALY as indicator of solidarity € 40.000 € 30.000 € 50.000 QALY A B C 28
Costs/QALY versus Burden of disease € 80.000 € 60.000 € 40.000 € 20.000 € 0 X X X X X Burden of disease 29
Dutch Council for Public Health and Health Care (RvZ, 2006) 30
If a medical treatment costs >€80,000 to give one patient one extra life year of good quality, it should not be reimbursed in the basic health care insurance Council advises the Minister of Health to use this limit in order to keep the budget of health care under control; They realize the topic is controversial.
Chris Murray • WHO avoid QALY • Havard • School of Public Health • Worked outside • Health economics • Med Decision Making • DALY • Person Trade-Off • Reinvented
Burden of disease: QALY lost = DALY (Disability adjusted life year) DALY QALY
Burden of disease expressed as “QALY lost” = DALY • Disability adjusted life years • The inverse of QALY • Used by the WHO • Expresses burden of disease • Measure of priority • More burden, more investment • QALY lost (DALY) = Measure of solidarity 34
QALY: both for effectiveness and solidarity • Evaluations assess cost-effectiveness in term of cost/QALY • But many decisions can not be explained by cost/QALY • Explanation in terms of fairness • People disagree with distributional implications of QALY maximisation • Fairness is burden of disease • Burden of disease is QALY lost (DALY) 35
QALY debate • Fairness is the issue in the QALY debate • QALY measurement is the straw man • Complex metric discussion • QALYs are needed to operationalize fairness • Most debate about quality of life assessment • Again as straw man • But also within the metric debate of QALY 36
Reimbursement arguments Burden of disease Effects Cost effectiveness
Alternative applications • Link to out of pocket payments • Greater out of pocket payments for conditions with lower proportional shortfall • E.g. France and Belgium • For example: • No reimbursement for the mildest conditions, such as common cold, acute tonsillitis, acute bronchitis, onychomycosis, tinea pedis • Partial reimbursement for conditions mild to moderate conditions: Haemorrhoids, candidiasis, gastritis, osteoporosis, erectile dysfunction, acne conglobata • Etc.
Take home message • Quality of life assessment and health assessment is crucial • Not only to estimate health gains (efficiency) • But also to estimate need (equity) • It is not the measurement of quality of life • but the efficiency/equity trade-off which heats up the debate