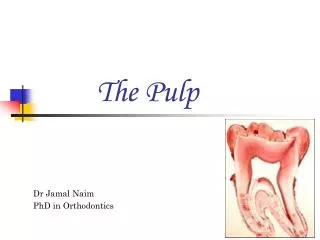
Direct Pulp Protection
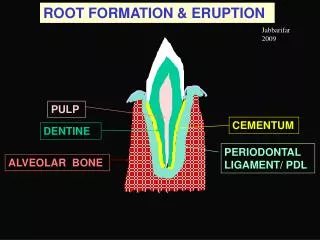
Direct Pulp Protection. Pulpotomy. Furcation Perforation. Radicular Reabsorption. Apexification. Root Perforation. Apexigenesis (Vital Root). Retro-Obturation. REPARING CEMENT. The treatment for accidents and endodontic complications. MTA- Angelus. 1. DESCRIPTION


Direct Pulp Protection
E N D
Presentation Transcript
Direct Pulp Protection Pulpotomy Furcation Perforation Radicular Reabsorption Apexification Root Perforation Apexigenesis (Vital Root) Retro-Obturation REPARING CEMENT The treatment for accidents and endodontic complications
MTA- Angelus • 1. DESCRIPTION • MTA-Angelus is an endodontic cement composed of several mineral oxides. It is indicated specially for root lateral trepanations treatment and furcation, internal re-absorptions, pareodontics surgeries, retro obturation, direct pulp protection, pulpotomy in incomplete root development teeth. • 1.1. Main Advantages: MTA-Angelus presents great advantages relating to amalgam and cements based on zinc oxide and eugenol: • Excellent marginal sealer which avoids bacterial migration and tissue fluids penetration to the interior of the radicular canal; • Radicular perforations biological enclosing and furcation enclosing through induction of peri-radicular cement formation; • Induction of dental barrier formation used upon the pulp; • Utilization in locals with presence of relative humidity, without lost of its properties. Different of other materials which demand an operatory field completely dry, normally difficult to get, principally in cases like pareodontics surgeries and retro-obturation.
2. USAGE TECHNIQUE To prepare medium size portion: one measure of MTA-Angelus powder + 01 drop of distilled water. a- Put one measure of powder and one drop of distilled water upon a sterilized glass plate; b- Spatulate both for 30 seconds until the perfect homogeneity of the components. The cement got must have a sandy consistency, similar to amalgam, but more humid; c- Insert the spatulated cement in the place desired, using a sterilized amalgam-place or another professional instrument of your preference; d- Condensate the material inside the dental cavity.
3. INDICATIONS AND TECHNICAL SURGERIES 3.1. RADICULAR CANAL PERFORATIONS OR FURCATION a. Anesthesia, isolating; b. Irrigation of the perforation area with sodium hypochlorite; c. Instrumentation, irrigation and obturation of the canal apex portion until the perforation area (Fig 01);
d. MTA-Angelus preparing, application into the perforation and condensation of the material with condensing equipments or with sterile cotton balls; (Fig. 02)
e. Obturation of the remnant of the radicular canal; (Fig. 03) f. Immediate radiographic control and after 3 to 6 months, in two years (at least).
Second section a – Calcium hydroxide removal with sodium hypochlorite; b – Obturation of the canal apex portion; c – MTA-Angelus preparation and fulfilling the re-absorption local using condensing equipments or sterile cotton balls; (fig.03) d – Immediate radiographic control and after 3 to 6 months for 2 years, at least. First section a – anesthesia, isolating; b – access to the canal and to the internal re-absorption area; (Fig. 01) c – irrigation with sodium hypochlorite; d – pulp and granulation tissue removal; e – curative application of calcium hydroxide paste [Ca(OH)2 + distilled water}. (Fig. 02) 3.2. RADICULAR PERFORATIONS TREATMENT BY INTERNAL RE-ABSORPTION (by means of canal)
c- Control of the hemorrhage area; d- MTA-Angelus preparation and application inside the dental cavity utilizing condensing equipments; (Fig.03) e- Material excess removal (do not irrigate it); f- Suture process and immediate radiographic control; g- Immediate Radiographic control and also after 3 to 6 months for at least 02 years. 3.3. Radicular Perforation Treatment (by means of surgery) The surgical procedure is indicated for the cases which a perforation realized by means were unsuccessful. Operational Technique a- Patch rising for localizing the perforation area; (Fig.01) b- Preparing of the perforation with burs in order to facilitate the material condensing process; (Fig. 02)
3.4. PAREODONTIC SURGERIES WITH RETRO-OBTURATOR MATERIAL Indicated for cases in which conventional endodontic treatment has failed or in cases of an impediment to the radicular canal by coronary means. Operational Technique a- Patch separation, ostectomy and radicular apex exposure.; (Fig. 01)
b- Radicular Resection from 2 to 3mm around the apex; (Fig.02) c- Class I retro-cavity preparation; d- Local humidity control;
e- MTA-Angelus preparation and application with an amalgam carrier and special apex condensing equipments; (Fig.03) f- Material excess removal (do not irrigate it); g- Hemorrhage induction from the periodontal junction and osseous tissue for the obturation exposure of the MTA-Angelus to the blood, aiming the hardening induction, which might happen in the presence of humidity; h- Suture process and immediate radiographic control; i- Radiographic Control after 3 to 6 months for at least 02 years.
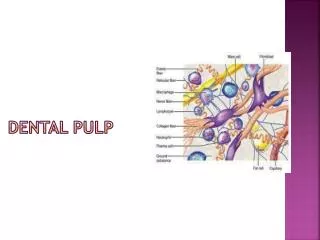
3.5. DIRECT PULP PROTECTION MTA-Angelus application upon the DPP pulp aims treatment of the pulp which was exposed by means of burs, caries or fractures. a- Anesthesia; b- Caries removal; c- Antisepsis of the cavity using sodium hypochlorite; d- MTA-Angelus preparation; e- Recovering of the local exposed area utilizing MTA-Angelus; f – Material covering and provisional restoration; g- Post-surgical control to verify the pulp vitality.
3.6. PULPOTOMY AND APEXIGENESIS* The surgical technique sequence is to be followed for both of the cases a- Anesthesia, absolute isolation; b- Access to the pulp chamber, pulp coronary removal and physiological serum irrigation; (Fig. 01) *Apexigenesis: : induction of the end of the root development portion inside vital teeth with a swollen coronary pulp.
c- Bleeding control; d- MTA-Angelus preparation and cement insertion upon the pulp utilizing a sterilized amalgam carrier; (Fig. 02)
e- Adaptation of the material applied utilizing a moisturized cotton ball; f- Protection of the material utilizing a sterilized cotton ball upon it; g – Provisionary Restoration (Fig. 03)
h- Clinical control in accordance with the symptoms and radiographic control from 3 to 3 months up to the end of the root development; i- After radicular formation is finished, either a conventional endodontic treatment or a coronary cavity restoration can be done. (Fig. 04)
3.7. APEXIFICATION* First Section: a- Anesthesia, complete isolation; b- Access to the pulp chamber, radicular canal odontometry and biomechanics, utilizing sodium hypochlorite for the irrigation process; (Fig. 01) * Inducing the development of the apex region hard tissue barrier on permanent young teeth utilizing incomplete developed roots with a necrotic pulp.
c- Insertion of Calcium Hydroxide paste utilizing distilled water as an intra-radicular curative for a week. (Fig. 02)
Second Section: a- Sodium Hypochlorite irrigation to eliminate the Calcium Hydroxide paste; b- Dry it with absorbent paper drying; c- MTA-Angelus preparation; d- Canal cement filling, condensating it up to the apex region, utilizing paper points or apex condensing, forming an apex tampon of 3 to 4mm; (Fig. 03)
e- Immediate radiography control to verify the correct canal filling procedure; f- Moisturized cotton ball placement upon the canal outlet; (Fig. 04)
g- Tooth restoration using a provisionary material for 24 hours. Third section: a- Provisionary restoration and cotton ball’s removal; b- Remnant radicular canal obturation, utilizing gutta-percha and conventional endodontic cement; (Fig. 05) *( TIP ) Important: A reinforcement on the canal walls are recommended if they happen to be too thin, utilizing composite resins for the canal filling;
c- Permanent restoration; d- Radiographic clinical control after 3 to 6 months until the development of a hard tissue barrier on the apical region. (Fig. 06)
4. COMPOSITION: SiO2 ,K20, Al2O3, Na2O, Fe2O3, SO3, CaO, Bi2O3,MgO and unsolved residues (crystalline silica, calcium oxide and potassium sulfate and sodium). 5. IMPORTANT PROPERTIES 5.1. Chemic-Physic Property In contact with water it becomes a little colloidal gum which solidify itself, forming a rigid structure in an interval of 10 minutes. 5.2. Hydrogeneization Potential (pH) Its PH is highly alkaline (12,0) avoids the bacterial growth, keeping its anti bacterial potential for a long period. 5.3. Radio-opacity The MTA-Angelus radio-opacity is superior than the dentine’s and bone tissue, and near to the guta percha’s, facilitating its visualization in operatory radiographic control and preservation.
It’s not necessary to wait for its hardening to continue the following procedures. One of the important MTA-Angelus characteristic is getting better results in humid places. In case of long procedures, the manipulated cement in the plate can harden, becoming difficult its utilization. For these situations, it is recommended to protect the cement with humid gauze. 5.4. HARDENING TIME The MTA-Angelus hardening time occurs in 10 minutes. 5.5. COMPRESSION RESISTANCE The compression resistance after 28 days is of 44,2 MPa. Its resistance is under very acceptable values, considering that it won’t have “direct” occlusal load in the applied areas. 5.6. SOLUBILITY It doesn’t present significant signals of solubility in contact with humidity, guaranteeing a excellent marginal closing.
5.7. SEALING POWER AND BACTERIAL MICRO-INFILTRATION The MTA-Angelus sealing power was tested through in vitro technique for evaluation of the coloring infiltration quantity in the dentine interface - MTA-Angelus. The result was a little grade of coloring infiltration. So, we conclude that the material presents a high sealing power, getting difficult the bacterial infiltration, once the bacterias have bigger dimensions than the coloring molecules.
Dear Dentist Surgeon The information referring to the product are based on clinical and scientific works. However, clinical success is subjected to a correct diagnostic, to a careful operatory technique, to local conditions of the treated tooth, as well as to the patient’s systemic situation. 5.8. EXTRAVASATING The presence of material outside de operatory cavity during the procedures of radicular perforation obturation, overcoming the periodontal linking, will result into an inflammation and traumatic lesion, consequently, delaying in the scar process. 5.9. RESISTANCE TO THE MOVEMENT MTA-Angelus has a good adherence capacity in the dentine walls becoming, by this reason, resistant to dislocation forces. It may also be indicated to furcation perforations. In this case it must be covered with a intermedium restoration material, before the final restoration material.