PULP PROTECTION
PULP PROTECTION. Cavity liners , varnishes and bases. CAUSES of Pulpal Injury :-. Ingress of Noxious products & bacteria through micro leakage (most common.) Thermal due to The heat produced by rotary instrument The heat conducted through restorative material.

PULP PROTECTION
E N D
Presentation Transcript
PULP PROTECTION Cavity liners , varnishes and bases
CAUSES of Pulpal Injury :- • Ingress of Noxious products & bacteria through micro leakage (most common.) • Thermal due to • The heat produced by rotary instrument • The heat conducted through restorative material. • Mechanical trauma due to cavity preparation. • Chemical irritation (by ingredients of materials) • Galvanic shock. This all results in a pulpal burn lesion an abscess formations or pulpal necrosis.
PULP PROTECTION caries Mechanical Thermal Chemical
OBJECTIVES FOR PULPAL PROTECTION • Pulpal protection requires consideration of • Chemical protection • Electrical protection • Thermal protection • Pulpal medication • Mechanical protection
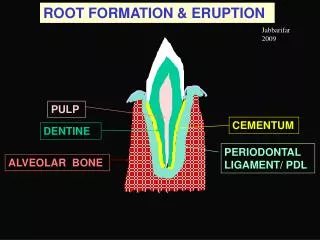
The dentin is capable of countering external stimuli if the remaining dentin thickness is 2.0 to 2.5 mm. In case, the remaining dentin thickness is less, pulp is to be protected using liner or base depending upon the amount of dentin left.
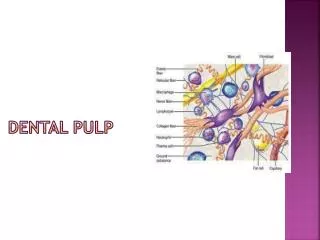
AFFECTED DENTIN: is the softened, demineralized dentin that is not yet invaded by bacteria. INFECTED DENTIN: is both softened and contaminated with bacteria. It includes the superficial, granular necrotic tissue and the softened, dry, leathery dentin. REMAINING DENTIN THICKNESS: it is the thickness of dentin from the pulpal extent of the cavity preparation to the pulp and is the single most important factor in protecting the pulp from insults.
CLASSIFICATION • CAVITY SEALERS provide a protective coating for freshly cut tooth structure of the prepared cavity. • a) varnish : a natural gum, such as copal rosin, or a synthetic resin dissolved in an organic solvent such as acetone, chloroform, or ether. Examples include Copalite, Plastodent Varnish, and Barrier • b) resin bonding agents : includes the primers and adhesives of dentinal and all-purpose bonding agents. Examples include All-Bond 2, Scotchbond MP+, Optibond, Probond, Amalgambond, etc
CAVITY LINERS : resin or cement coating of minimal thickness (usually less than 0.5 mm) to achieve a physical barrier and/or therapeutic effect (a chemical effect that in some way benefits the health of the tooth pulp). Examples include Dycal, Life, Cavitec, Hydroxyline, Vitrebond and Fuji Lining LC • CAVITY BASES : A replacement material for missing dentinal tooth structure, used for bulk buildup and/or for blocking out undercuts.
Cavity Liners, Bases, Varnishes. Liners and bases are materials placed between dentin and the restoration to provide pulpal protection Liners are relatively thin layers of materials used primarily to provide a barrier to protect the dentin from residual reactants diffusing out of a restoration and or oral fluids that may penetrate leaky teeth, Restoration interfaces.
Cavity Varnish: Cavity varnish is a solution of one or more resins which when applied onto the cavity walls, evaporates leaving a thin resin film, that serves as a barrier between the restoration and dentinal tubules
is a mixture of Copal resin & organic solvent and on application the solvent evaporates, leaving a resin layer over dentin. • This seals dentinal tubules • better marginal adaptability. • Two coats of varnish are considered sufficient since Varnish is hydrophobic • 1st coat application 55 % wetting is achieved (smear layer has moisture) • 2nd coat application 85 – 90 % wetting is achieved. Functions :- • Prevents micro leakage • Reduce post operative sensitivity. • Reduce diffusion of acid from cement into dentin.
Applications: • It reduces microleakage around the margins of newly placed amalgam restorations, thereby reducing post-operative sensitivity • It reduces passage of irritants into the dentinal tubules from the overlying restoration or base. • In case of amalgam restorations, they prevent penetration of corrosion products into the dentinal tubules thus minimising tooth discolouration
It may be used as a reinforce coating over certain restorations to protect them from dehydration or contact with oral fluids. • May be applied on the surface of metallic restorations as temp. protection in case of galvanic shock. • In case where electro surgery is done adjacent to metallic restorations, varnish applied over the restoration serves as a temp electric insulator
Composition: It is a natural gum such as copal, resin or synthetic resin dissolved in an organic solvent such as alcohol ,acetone or ether Medicinal agents such as chlorbutanol, thymol and eugenol may be added. Some varnishes also certain fluoride.
Properties: The film thickness ranges between 2-4mm. They neither possess mechanical strength nor provide thermal insulation because of thin film thickness The solubility of dental varnish is low. They are virtually insoluble in distilled H2O
Manipulation: The varnish can be applied using a brush, wire loop or a small pledget of cotton. Several thin layers are applied. Each layer is allowed to dry before applying the next, when the 1st layer dries, small pin holes develop. There voids are filled in the succeeding varnish applications to attain a uniform and continuous coating.
Precautions: • Varnish solutions should be tightly capped immediately after use to prevent loss of solvent by evaporation. • It should be applied in thin consistency. Viscous varnish does not reset the cavity walls properly. It should be thinned with an appropriate solvent. • Excess varnish should not be left on the margin of the restorations [prevents proper finishing of the margins of the restoration.
Clinical considerations: 1. When placing a silicate or silicophosphate restoration the varnish should be confined to the dentin. varnish applied to the enamel would inhibit the release of fluoride by enamel.
2. Contra Indications: • Composite Resin: The solvents in the varnish may react with or soften the resin • GIC – varnish eliminates the pottential for adhesion and biocompatibility of the cement • When therapeutic action is expected from the overlying cement • Eg: (ZnOE & Ca(OH)2
Cavity varnish should be applied • AFTER • Ca(OH)2 containing preparations • ZOE cement • Carboxylate cement • GIC cement • BEFORE • ZnPO4 cement • Zn Silicophosphate cement • Silicate cement • Amalgam • Gold foil
Cavity Liner: A cavity liner is used like a cavity varnish to provide a barrier against the passage of irritants from cements or other restorative materials and to reduces the sensitivity of freshly cut dentin. They are usually suspensions of Ca(OH)2 in a volatile solvent on evaporation of the volatile solvent, the liner forms a thin film on the prepared tooth surface. Composition: Suspension of Ca(OH)2 in an organic liquid such as methyl ethyl ketone or ethyl alcohol.
They can be classified as • Thin film liners (1-50mm) • Solution liners Suspension liners • (Varnishes 2 to 5mm) (20 – 25mm) • Thick Liners (200 –1000mm) • Primarily selected for pulpal medication and thermal protection. • Bases.(1-2mm) – used to provide thermal insulation
IDEAL REQUIREMENTS OF CAVITY LINERS • Bacteriostatic • Provide electrical & thermal insulation • Prevent discolouration of tooth structure • Prevent penetration of chemical ions from the restorative materials to dentin and pulp • Prevent marginal leakage at the tooth restoration interface • Anticariogenic property • Chemical bonding to tooth structure
Properties: Like varnishes, cavity liners neither possess mechanical strength nor provide significant thermal insulation. Ca(OH)2 are soluble and should not be used at the margins of the restoration Fluoride compounds have been added to some liners to reduces the possibility of sec. caries around permanent restoration.
Cement Base: • A base is a layer of cement placed under the permanent restoration to encourage recovery of the injured pulp and to protect it against numerous types of insult to which it may be subjected. • It serves as replacement or substitute for the protective dentin, that has been destroyed by caries or cavity preparation. • Types: • A variety of materials may be employed in general they belong to 2 categories • Low strength Bases • High strength Bases
The base is applied only on the pulpal & the axial walls & not on other walls of the preparation because all cements by & large dissolve in oral fluids (quantity may vary) this dissolution may lead to spacing at tooth restoration interface micro-leakage. Therefore avoided on the walls which are open to oral environment • Base thickness 0.5mm
The following are guidelines for the placement of bases • Do not remove sound tooth structure to provide space for a base. This will maximize sound tooth structure for restoration support and RDT for pulpal protection • Minimize the extent of the base. Basing a preparation to “ideal” depth and outline form is contraindicated. This leads to decreased bulk of restorative material and increased potential for restoration fracture
Use the minimum thickness necessary to achieve the desired result. This should not exceed 0.5 – 0.75 mm under amalgam restorations • Currently, there is not yet any convincing evidence for the routine use of bonding agents under metallic restorations
Selection of suitable cement as a base depends on : • 1) design of the cavity • 2) type of permanent restorative material • 3) proximity of pulp in relation to the cavity floor
CLASSIFICATION OF CEMENT BASESACCORDING TO STRENGTH PROPERTIES • LOW STRENGTH BASES • - Ca(OH)2 CEMENTS • - ZOE CEMENT • - (used as pulp capping) • HIGH STRENGTH BASES • - ZnPO4 CEMENT • - Zn POLCARBOXYLATE CEMENT • - GIC • - (provide thermal, electrical insulation & mechanical support to restorative materials)
ACCORDING TO ITS CHEMICAL NATURE OR pH • ACIDIC : GIC, ZnPO4, ZnPolycarboxylate cements • NEUTRAL : ZOE cements • ALKALINE : Ca(OH)2 cement
ACCORDING TO METHOD OF DISPENSING • 2 PASTE SYSTEM : Ca(OH)2 cement and ZOE cements • POWDER-LIQUID SYSTEM : ZOE cements, ZnPO4, ZnPolycarboxylate cement, Ca(OH)2 cement • SINGLE PASTE SYSTEM : Light activated Ca(OH)2 cement
Properties: Thermal Properties: The base must provide thermal protection to the pulp For effective thermal protection the base should have minimal thickness of 0.5 to 0.75mm
Protection against chemical insults. The cement base also serves as a barrier against penetration of irritating constituents (acids, monomer etc) from restorative materials. Ca(OH)2 and ZnOE are most effective for this.
Therapeutic effect: Ca(OH)2 acts as a pulp capping agent and promotes the formation of secondary dentin. ZOE has an obtundant effect on pulp strength. The base should have sufficient strength to withstand the forces of condensation without fracture under masticatory stresses. It should develop strength rapidly in order to allow early condensation of amalgam.