VITAL PULP THERAPY
VITAL PULP THERAPY. Includes: Indirect Pulp Therapy Direct Pulp Cap Pulpotomy Apexification. VITAL PULP THERAPY. Endodontics: The PREVENTION or Treatment of Apical Periodontitis. INDIRECT PULP THERAPY. Also called indirect pulp cap DEFINITION:


VITAL PULP THERAPY
E N D
Presentation Transcript
VITAL PULP THERAPY • Includes: • Indirect Pulp Therapy • Direct Pulp Cap • Pulpotomy • Apexification
VITAL PULP THERAPY Endodontics: The PREVENTION or Treatment of Apical Periodontitis
INDIRECT PULP THERAPY • Also called indirect pulp cap • DEFINITION: • Placement of protective dressing over thin remaining dentin which, if removed, might expose the pulp • PURPOSE: • To protect the pulp from further injury and to permit healing and repair
INDIRECT PULP THERAPY • INDICATIONS: • Primary and permanent teeth • Minimal pulpal inflammation • No clinical signs of pulpal degeneration • Asymptomatic or symptoms of reversible pulpitis • Sharp, fleeting pain to thermal, osmotic stimuli • No spontaneous pain • Responds WNL to thermal and electric pulp tests • No radiographic signs of periapical inflammation • No widened pdl • No p/a radiolucency
INDIRECT PULP THERAPY • SUCCESS RATE • 99% success for avoiding pulpexposure • 92% success – 3½-4½ year follow-up • Failed indirect pulp therapy means irreversible pulpal disease
INDIRECT PULP THERAPY • TECHNIQUE • Anesthetic • Rubber dam to keep bacterial count as low as possible • Remove all caries at DEJ and just enough remaining caries to permit placement of a temporary restoration • Large round bur less likely to cause accidental exposure than spoon excavator
INDIRECT PULP THERAPY • TECHNIQUE (cont’d) • Place ZOE dressing (can also use CaOH) • SEAL with IRM (toxic to bacterial cells) • SEALING is the most important step • Can use Amalgam or Glass Ionomer if longer term seal is required
INDIRECT PULP THERAPY • TECHNIQUE (cont’d) • After 8 weeks, remove remaining caries, evaluate: arrested? exposure? • If no pulp exposure – final restoration • If pulp exposure – direct pulp cap or pulpotomy or pulpectomy • Failed Indirect Pulp Cap means irreversible pulpal disease
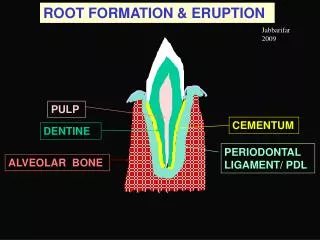
INDIRECT PULP THERAPY • NOTE re: IMMATURE TEETH • Indirect pulp cap should be used whenever possible to avoid pulp exposure. In immature teeth (open apices) every attempt must be made to maintain pulp vitality until root development is complete. Loss of vitality before complete root development leaves a short, thin, weak root more prone to fracture, poorer crown:root ratio. ALWAYS TRY TO AVOID APEXIFICATION IF APEXOGENISIS IS POSSIBLE
DIRECT PULP CAP • DEFINITION: • Placement of a protective dressing directly over pulp at site of exposure • PURPOSE • To permit healing & repair and to maintain the pulp’s vitality and function
DIRECT PULP CAP • INDICATIONS: • Permanent teeth only • Carious or mechanical exposures ie. when indirect pulp therapy fails or in the RARE event of an accidental exposure • Best used on teeth with immature permanent with exposed pulps • Once root formation is complete – NSRCT • Use in mature teeth is controversial. Best considered a temporary or compromise tx
DIRECT PULP CAP • INDICATIONS (cont’d) • Careful Case Selection: • Minimal pulpal inflammation • No clinical signs of pulpal degeneration • No radiographic signs of p/a inflammation • Young pulp better prognosis • No pulp calcifications better • Little or no bleeding at exposure site • Mechanical better than carious
DIRECT PULP CAP • INDICATIONS (cont’d) • Small exposure better • Location of exposure – axial wall worse • No purulent or serous exudate at exposure • BUT REMEMBER: a pulp with no signs or symptoms is not always a healthy pulp (stressed)
DIRECT PULP CAP • SUCCESS RATE: Controversial • Depends of definition of success • High success rate if judged by absence of clinical signs and symptoms • Low success rate based on presence of chronic inflammation on histologic exam
DIRECT PULP CAP • SUCCESS RATE (cont’d) • Higher success rate in short term • Long term – persisting pulpal inflammation. May lead to calcification, internal or external resorption which complicates future NSRCT • Therefore: IDEAL treatment for all carious exposures in mature permanent teeth is NSRCT
DIRECT PULP CAP • TECHNIQUE: • Calcium Hydroxide is material of choice • Dycal etc. • Marginal seal is critical • Careful caries removal to avoid forcing dentin debris and micro-organisms into pulp
DIRECT PULP CAP • MECHANISM OF ACTION: • CaOH causes necrosis of superficial pulp and inflammation of contiguous tissue. • Dentin bridge formation occurs at junction of necrotic and inflamed vital tissue. • Dentin bridge consists of superficial bone-like layer and deeper dentin-like layer. • Blood clot inhibits bridge formation
DIRECT PULP CAP • MECHANISM OF ACTION (cont’d) • Radiographic studies of radiolabeled CaOH have shown that Ca in dentin bridge comes from blood – not from CaOH • Bridge - irregular porous tubular dentin • Becomes thicker & less permeable with time • Exact mechanism of action unknown BUT certain concentrations of CaOH known to be mitogenic for pulp fibroblasts (odontoblast replacement cells)
PULPOTOMY • DEFINITION: • The surgical amputation of the coronal portion of an exposed pulp • PURPOSE: • To protect and preserve the remaining radicular pulp’s vitality and function
PULPOTOMY • INDICATIONS: • Exposed vital pulps in carious primary teeth • Exposed vital pulps in carious immature permanent teeth (to allow continued root development prior to NSRCT) • Traumatically exposed primary or permanent teeth; mature or immature • As an emergency procedure prior to NSRCT
PULPOTOMY • PROGNOSIS: • Questionable in carious exposures in mature teeth. • Good for apexogenisis in immature teeth with carious exposures • Excellent for traumatic exposures regardless of root maturity, size of exposure or time elapsed since injury
PULPOTOMY • TECHNIQUE: • Carious Exposure: • Pulp removed to cervical line in anterior teeth, to canal orifices in posterior teeth • Clinical judgement influences amount of tissue removed • High speed diamond with water spray • Care to remove all shreds of pulp coronal to amputation site
PULPOTOMY • TECHNIQUE (cont’d) • Flush with sterile saline • Do Not air dry • Control hemo with moist cotton pellets and gentle pressure for approx. 5 min. • If hemo cannot be controlled, amputation should be performed at a more apical level • If hemo still continues in immature tooth control with hemostatic agents eg. aluminum chloride or ferric sulfate (compromise treatment)
PULPOTOMY • TECHNIQUE (cont’d) • Place CaOH dressing – do not use hard setting CaOH deep in canals – use CaOH powder • Base – usually IRM or other cement • Marginal seal of final restoration critical • Regular follow-up until root development complete and NSRCT may be performed
PULPOTOMY • TECHNIQUE (cont’d) • Traumatic Exposure: • Cvek Pulpotomy: • Mature or immature teeth • Remove only 2-3mm of pulp • Place CaOH (eg. Dycal) • No further endodontic treatment is usually required • 91% success at 4 year follow-up
Open Apex OPEN APEX CASES Vital Pulp Necrotic pulp Apexogenisis Apexification
OPEN APEX CASES • APEXOGENISIS • Treatment: • Indirect Pulp Cap • Direct Pulp Cap • Pulpotomy
OPEN APEX CASES • APEXOGENISIS • Materials: • CaOH • Bonded Materials (resins, GICs) • MTA
OPEN APEX CASES • APEXIFICATION: • Indication: Immature tooth with necrotic pulp • Traditional Technique: Canal disinfection (instrumentation, irrigation, CaOH dressing); replace dressing periodically over 1-3 years; formation of apical dentin barrier; obturation • Alternate Technique: Canal disinfection (instrumentation, irrigation, CaOH dressing); place MTA apical barrier after 1 week (microscope); obturate with gutta-percha and sealer.