Nursing Management: Congestive Heart Failure
480 likes | 2.95k Vues
Congestive Heart Failure. More than deaths from heart disease are due to end stage CHF"The American Heart Association estimates that 400,000 new cases of CHF occur each year"The 5 year mortality rate for CHF is about 50%"Lewis. Congestive Heart Failure. In the past 15 years deaths fro

Nursing Management: Congestive Heart Failure
E N D
Presentation Transcript
1. Nursing Management: Congestive Heart Failure Nurs1228
Spring 2003
By Nina Green, RN
2. Congestive Heart Failure �More than � deaths from heart disease are due to end stage CHF�
�The American Heart Association estimates that 400,000 new cases of CHF occur each year�
�The 5 year mortality rate for CHF is about 50%�
Lewis
3. Congestive Heart Failure �In the past 15 years deaths from CHF have increased 116%�
The rate of sudden cardiac death in a patient with CHF is 6 to 9 times higher than for the general population
Lewis
4. Congestive Heart Failure �About 20% of individuals who have a heart attack will be disabled with heart failure within 6 years�
�CHF is the single most frequent cause of hospitalization for people age 65 or older�
Lewis
5. Risk Factors for CHF Coronary artery disease
Hypertension
High cholesterol levels Advancing age
Cigarette smoking
Obesity
Proteinuria
Diabetes
6. Normal mechanisms regulating Cardiac Output Preload volume
Afterload volume
Heart rate Myocardial contractility
Metabolic state of the individual
7. Major causes of CHF Underlying cardiac disease
Congenital
acquired Precipitating causes
Increase workload of ventricles
Leads to decreased myocardial function
8. Acute cardiac disease causing CHF Acute MI
Pulmonary Emboli
Hypertensive crises
Ventricular septal defect Arrhythmias
Thyrotoxicosis
Rupture of papillary muscle
9. Chronic cardiac disease causing CHF Coronary artery disease
Rheumatic heart disease
Cor pulmonale
anemia Hypertensive heart disease
Congenital heart disease
Cardiomyopathy
Bacterial endocarditis
10. Precipitating causes of CHF Anemia
Thyrotoxicosis
Arrhythmias
Pulmonary embolism
Paget�s disease
hypervolemia Infection
Hypothyroidism
Bacterial endocarditis
Pulmonary disease
Nutritional deficiencies
11. Pathology of Ventricular Failure Systolic failure: causes ventricle not to empty properly (most common cause of CHF)
Heart muscle has decreased ability to contract
Also caused by increased afterload (hypertension), or mechanical abnormalities ( like valvular heart disease)
Characterized by low forward blood flow
12. Pathology of Ventricular Failure Diastolic failure: causes ventricle not to fill properly
Disorder of heart relaxation and ventricular filling
Usually the result of ventricular hypertrophy
Caused by chronic hypertension, aortic stenosis, or cardiomyopathy
Commonly seen in older adults
13. Compensatory Mechanisms of the heart in CHF Ventricular dilation
Increased sympathetic nervous system stimulation Ventricular hypertrophy
Hormonal response (Renal response)
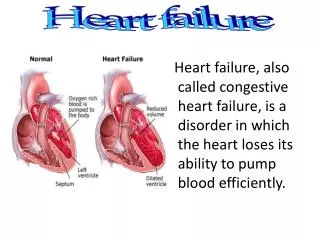
14. Types of CHF Left sided failure
Back up of blood into the lungs
Common causes are: CAD, HTN, cardiomyopathy and rheumatic heart disease
Other causes can be: MI damage, ischemia, scar tissue (reducing contractility),
15. Types of CHF Right sided failure
Backup of blood into the venous system and right side of the heart
Primary cause is left sided failure
Also caused by Cor pulmonale (caused by COPD, and pulmonary emboli)
Also caused by MI damage, ischemia and scarring
16. Clinical manifestations of Acute CHF Pulmonary edema (Most prominent)
Caused by left sided failure
Evidenced by:
Agitation
Paleness or cyanosis
Clammy cold skin
Severe dyspnea with use of accessory muscles
Respiratory rate > 30/min
Coughing, wheezing, production of frothy blood- tinged sputum
17. Manifestations of Chronic CHF Fatigue
Tachycardia
Edema
Nocturia
Weight changes
Dyspnea
Skin changes
Behavioral changes
Chest pain
18. Complications of Congestive Heart Failure Pleural effusion
Increased pressure in pleural capillaries
Leakage of fluid from capillaries into pleural space.
Arrhythmias
Left ventricular thrombus
Hepatomegaly
Liver becomes congested with venous blood
Leads to impaired liver function
19. Nursing Care in Acute CHF Decrease the intravascular volume
With use of diuretics
Decrease the venous return
Reduces congestion in heart and lungs
Sitting patient up facilitates breathing
Decreasing the afterload
Use of vasodilators (IV Nipride)
Increasing myocardial contraction and CO
Reducing pulmonary congestion
20. Nursing Care of Acute CHF Improve Gas Exchange and Oxygenation
Give IV morphine
Place on Oxygen
Intubate and place on vent as needed
Improve cardiac function
Digitalis, or newer inotropic drugs (dobutamine) increase cardiac contractility
Hemodynamic monitoring
21. Nursing Care of Acute CHF Reduce anxiety
Give Morphine
Approach patient calmly
Remember: Nursing care will focus on continual physical assessment of the patient, hemodynamic monitoring, and monitoring the patient�s response to the treatment.
22. Nursing Care of Chronic CHF Treatment is aimed at resolving the underlying problem (Physicians job)
Arrhythmias (medication, and defibrillator implants), hypertension (medication), valvular defects (surgery), ischemic heart disease (cardiac cath, CABG,�),
Need for oxygen
Need for physical and emotional rest
23. Nursing Care of Chronic CHF Drug therapy includes:
Sodium-potassium-ATPase inhibitors
Digitalis (Lanoxin)
B-Adrenergic agonists
Dopamine (Intropin)
Dobutamine (Dobutrex)
Phosphodiesterase inhibitors
Amrinone (Inocor)
Milrinone (Primacor)
24. Nursing Care of Chronic CHF Diuretics:
Lasix, Edecrin, Bumex, and Demadex
Aldactone and Dyrenium used also, because they are potassium sparing
Vasodilators:
Nipride (IV) (usually in ICU) and nitroglycerine (often in paste form)
25. Nursing Care of Chronic CHF Angiotensin-converting enzyme (Ace) inhibitors:
Capoten, Vasotec, lisinopril (Prinivil, Zestril)
Reduces angiotension II and plasma aldosterone levels
Increases cardiac output due to vasodilitation
Beta-adrenergic blocking agents:
Coreg (is the only beta-blocker used in mild to moderate CHF)
26. Nursing Care of Chronic CHF Nutritional Therapy
Sodium restriction with diet
Teach patient what foods are high in sodium and to avoid them
Severe CHF has the most sodium restrictive diet
instruct family in reading labels on food items
Fluids may be restricted in moderate to severe CHF
27. Nursing Assessment Subjective data:
Past health history
Medications
Functional health patterns
Health perception-health management: (fatigue?)
Nutritional-metabolic: (usual sodium intake, etc�)
Elimination: (nocturia?)
Activity-exercise: (dyspnea?)
Sleep-rest: (nocturnal dyspnea?)
Cognitive-perceptual: (chest pain?)
28. Nursing Assessment Objective data:
Skin
Respiratory system
Cardiovascular system
Gastrointestinal system
Neurologic system
Lab values
Hemodynamic monitoring
Other tests: chest x-ray, echocardiogram, etc...
29. Nursing Diagnoses Activity intolerance r/t�..
Sleep pattern disturbance r/t�.
Fluid volume excess r/t�
Risk for impaired skin integrity r/t�
Impaired gas exchange r/t�
Anxiety r/t�
Ineffective management of therapeutic regimen r/t� (See Text pg 900-901)
30. Nursing Interventions Regular assessment of patients level of fatigue, dyspnea, heart rate, and weight
Provide emotional and physical rest
Provide frequent small feedings
Teach patient energy expenditure and how to self monitor activities for appropriateness
Teach patient reasons for nocturnal dyspnea
31. Nursing Interventions Help patient explore alternative positions for comfortable sleep and relief of dyspnea
Teach patient to take diuretics early in day to prevent having to get up at night
Give all meds as ordered
Monitor intake and output
Monitor for signs of peripheral edema or lung congestion
32. Nursing Interventions Instruct patient to weigh daily and to keep a record of their weights
Monitor patient for signs and symptoms of hypokalemia
Provide client with a diet that is sodium restricted as ordered by physician
If patient has edema, measure and record
Assess edematous sites for skin breakdown
33. Nursing Interventions Perform passive ROM to extremities q 4h
Handle edematous skin gently
Turn and reposition q 2 h
Monitor for impaired breathing
Position HOB up if having difficulty breathing
Give O2 if needed by nasal cannula
Use pulse ox prn
34. Nursing Interventions Assess heart and lung sounds q 4-8 h and prn
Assess patient for anxiety. Medicate as needed
Allow patient to ask questions and verbalize concerns.
Explain all procedures to patient in understandable terms
Respond to call light quickly
35. Nursing Interventions Use measures to decrease dyspnea for patient, thereby relieving anxiety r/t breathing difficulty
Use calm behavior with patient
Teach patient what to report to nursing staff, shortness of breath, edema/swelling in ankles, weight gain,�etc�
Teach patient and family about sodium restricted diet
36. Ambulatory and Homecare Educate patient and family about the physiologic changes that have occurred
Assist the patient to adapt to the physiologic and psychologic changes that have occurred. (Include family in this.)
Home health nursing care is a vital factor in the prevention of future hospitalizations for these patients.
37. Ambulatory and Homecare The homecare nurse can follow up with ongoing clinical assessments of the patient, monitor vital signs, and response to therapy (including medication).
See table 33-13 of Text on pg. 902