Download
1 / 1
10 likes | 116 Vues
Yield of colonoscopy for advanced neoplasia in a population-based setting. Bernard DENIS, Jacques PICOT, Jean François VIES, Marjorie MUSSO, Paul François FOURNIER, Frédéric VAGNE, Jean Louis COLSON, Isabelle GENDRE, Philippe PERRIN.

E N D
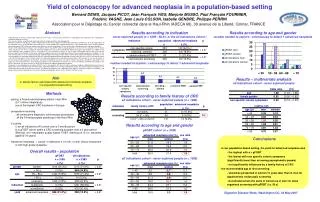
Yield of colonoscopy for advanced neoplasia in a population-based setting Bernard DENIS, Jacques PICOT, Jean François VIES, Marjorie MUSSO, Paul François FOURNIER, Frédéric VAGNE, Jean Louis COLSON, Isabelle GENDRE, Philippe PERRIN Association pour le Dépistage du Cancer colorectal dans le Haut-Rhin (ADECA 68), 39 avenue de la Liberté, Colmar, FRANCE Abstract Results according to age and gender number needed to explore / colonoscopy to detect 1 advanced neoplasia Results according to indication never explored people (n = 1099 - 50.4% of the all indications cohort ) Implementation of universal colonoscopic colorectal cancer (CRC) screening and surveillance is inappropriate and impossible. Risk stratification is needed for targeted screening. Aim: to assess factors associated with advanced colorectal neoplasia within a defined population. Methods: prospective recording of 2 cohorts composed of all consecutive diagnostic colonoscopic procedures performed by all the 34 endoscopists of the Haut-Rhin area: 1) an all indications (AI) cohort over a 3 month period and 2) a gFOBT cohort over a 3 year period within a CRC screening program with guaiac-based FOBT. Advanced neoplasia was defined as cancer or adenoma ≥ 10 mm, or with villous component or with high-grade dysplasia. Results: 5568 colonoscopic procedures were recorded: 3185 in the gFOBT cohort in people aged 50 to 74 (men 54.7%) and 2383 in the AI cohort (mean age 58.9 y, men 48.1%). Overall, the advanced neoplasia rate was 31.0% in the gFOBT cohort and 12.5% in the AI cohort (p < 0.0001). In the latter, indications were symptoms (56.5%), screening (23.5%) and surveillance (20.0%). In the AI cohort, 1099 people (50.4%) had never had any previous colorectal examination. In this group, advanced neoplasia rates were not significantly different between people explored for symptoms (11.4%) and screening (10.6%). In the symptomatic group, abdominal pain and change in bowel habits had the lowest advanced neoplasia rate (6.0%). In the screening group, the advanced neoplasia rate was not significantly different between people with a family history of CRC, even in a first-degree relative < 60 y (9.2%) and without (19.4%). In both cohorts, the advanced neoplasia rate increased with age and was 1.9 time higher in men than in women. In the previously unexplored group of the AI cohort, the advanced neoplasia rate was low in women, similar in the 40-49 y and 50-59 y age groups (3.8% and 3.9%) and increased to 10.1% in the 60-69 y age group. It was respectively 8.5% and 21.3% in men in the 40-49 y and 50-59 y age groups. In the 40-59 y age group, men were four times as likely to have advanced neoplasia compared with women. Conclusion: in our population-based setting, gFOBT is by far the indication with the best yield for advanced neoplasia. Abdominal pain and change in bowel habits are the indications with the lowest yield, significantly lower than screening asymptomatic people. The yield for advanced neoplasia is not significantly influenced by a family history of CRC. The advanced neoplasia rate is about four times higher in men than in women in the 40-59 y age group and the recommended age at first screening should be postponed in women at least 10 years later than in men. number needed to explore / colonoscopy to detect 1 advanced neoplasia Aim to assess factors associated with advanced colorectal neoplasia in a population-based setting Results – multivariate analysis all indications cohort - never explored people Methods Results according to family history of CRC all indications cohort - never explored people (n = 1099) • setting: a French administrative district: Haut-Rhin • (0.71 million inhabitants) • one of the highest CRC incidence in Europe • prospective recording • . all consecutive diagnostic colonoscopic procedures • . all the 34 endoscopists practicing in the Haut-Rhin • - 2 cohorts • 1) an all indications (AI) cohort over a 3 month period • 2) a gFOBT cohort within a CRC screening program over a 3 year period • (Biennial non rehydrated guaiac-based FOBT (Hemoccult II) for residents aged 50-74 years) • - Advanced neoplasia = cancer or adenoma ≥ 10 mm, or with villous component or with high-grade dysplasia. Results according to age and gender gFOBT cohort(n = 3185) Conclusions in our population-based setting, the yield for advanced neoplasia was - the highest with a + gFOBT - the lowest with non specific colonic symptoms (significantly lower than screening asymptomatic people) - not significantly influenced by a family history of CRC the recommended age at first screening - should be postponed in women 10 years later than in men for opportunistic endoscopic screening - but should remain the same in women as in men for mass organized screening with gFOBT (i.e. 50 y) Overall results - population all indications cohort - never explored people (n = 1099) Digestive Disease Week, Washington DC, 22 May 2007