Download
1 / 32
320 likes | 485 Vues
ANDALIB.A.MD ALZAHRA HOSPITAL. MECHANISM OF MENISCi AND LIGAMENTs INJURY. medial meniscus.

E N D
ANDALIB.A.MD ALZAHRA HOSPITAL MECHANISM OF MENISCiAND LIGAMENTs INJURY
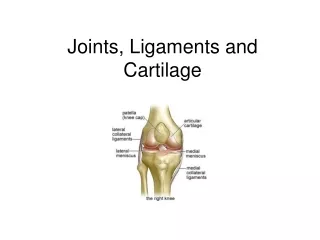
medial meniscus The medial meniscus is a C-shaped structure larger in radius than the lateral meniscus, with the posterior horn being wider than the anterior. The anterior horn is attached firmly to the tibia anterior to the intercondylar eminence and to the anterior cruciate ligament
LATERAL MENISCUS • The lateral meniscus is smaller in diameter, thicker in periphery, wider in body, and more mobile than the medial meniscus. It is attached to both cruciate ligaments and posteriorly to the medial femoral condyle by either the ligament of Humphry or the ligament of Wrisberg, depending on which is present; it is also attached posteriorly to the popliteus muscle
The lateral meniscus is smaller and more mobile than the medial meniscus. The inner portion of the menisci are avascular. The outer portion has some blood supply, making healing of tears possible. lateral medial
MENISCUS TEARING The menisci follow the tibialcondyles during flexion and extension, but during rotation, they follow the femur and move on the tibia. the medial meniscus becomes distorted. Its anterior and posterior attachments follow the tibia, but its intervening part follows the femur; thus it is likely to be injured during rotation
LATERAL MENISCUS • because it is firmly attached to the popliteus muscle and to the ligament of Wrisberg or of Humphry, follows the lateral femoral condyle during rotation and therefore is less likely to be injured.
Meniscal Lesions • Most common MOI is rotary force with knee flexed or extended • Tears may be longitudinal, oblique, or transverse • Medial meniscus is more commonly injured due to ligamentous attachments and decreased mobility • Also more prone to disruption through torsional and valgus forces
Mechanisms of injury • An acute twisting injury from impact during a sport • Usually the foot stays fixed on the ground and the rest of body rotates • Getting up from a squatting or crouching position • Loading the knee from a fixed position
MENUSCAL TEARING ARTHROSCOPIC VIEW • B, Horizontal tear of degenerative lateral meniscus. • C, Oblique tear of posterior horn of lateral meniscus. • D, Incomplete radial tear of lateral meniscus. • E, Degenerative tear of lateral meniscus. • F, Resection of tear of lateral meniscus. Remaining tissue shows fatty degeneration.
Four mechanisms have been described as capable of disrupting the ligamentous structures around the knee: abduction, flexion, and internal rotation of the femur on the tibia; (2) adduction, flexion, and external rotation of the femur on the tibia; (3) hyperextension;, and (4) anteroposterior displacement
LIGAMENT INJURY By far the most common mechanism is abduction, flexion, and internal rotation of the femur on the tibia when the weight bearing leg of an athlete is struck from the lateral aspect by an opponent.
the unhappy triad” of O'Donoghue the medial collateral ligament and the medial capsular ligament—are the initial structures injured. If the force is of sufficient magnitude, the anterior cruciate ligament also can be torn. The medial meniscus may be trapped between the condyles of the femur and the tibia, and it may be torn , thus producing “the unhappy triad” of O'Donoghue
The mechanism of adduction, flexion, and external rotation of the femur on the tibia is much less common and produces the primary disruption laterally • The lateral collateral ligament usually is disrupted initially, and depending on the magnitude of the trauma and displacement, the capsular ligaments, the arcuate ligament complex, the popliteus, the iliotibial band, the biceps femoris, the common peroneal nerve, and one or both cruciate ligaments may be disrupted.
hyperextension mechanism • Force directed to the anterior aspect of the extended knee, a hyperextension mechanism, usually injures the anterior cruciate ligament, and if the force continues or is severe, stretching and disruption of the posterior capsule and posterior cruciate ligament may result.
hyperextension mechanism • Mechanisms reported as possibly able to disrupt the anterior cruciate ligament with minimal injury of other supporting structures are hyperextension, marked internal rotation of the tibia on the femur, and pure deceleration
all the supporting structures around the knee function in concert • no single ligament can be disrupted without some degree of injury being sustained to other supporting structures. Injury to the other structures may be minimal and thus may heal with conservative measures, leaving what is apparently an isolated injury to clinical examination.
Isolated posterior cruciate disruption can result from a direct blow to the front of the tibia with the knee flexed.
PCL Injuries • When the knee is forcefully twisted or hyperextended BUT other ligaments are usually injured or torn, before the posterior cruciate ligament (PCL) is torn • Most common mechanism for PCL alone to be injured is from a direct blow to the front of the knee while the knee is bent. • Automobile accident • Automobile strikes another and stops suddenly • Front passenger or driver slides forward. • Bent knee hits the dashboard just below the knee cap forcing tibia backwards on the femur tearing PCL. • The same force can occur during a fall on the bent knee, where the force of the fall on the tibia pushes it back against the femur and tears the posterior cruciate ligament (PCL).
Common mechanism of PCL injury in football is being tackled while the knee is fully extended. When the tibia is displaced too much in the posterior direction the PCL may rupture.
Gender issues related to ACL injuries females more likely to sustain an ACL injury than males soccer - 2.6X basketball - 5.75X wider pelvis greater flexibility less-developed musculature hypoplasticvastusmedialisobliquus narrow femoral notch genuvalgum external tibial torsion
L M Ligament Injuries • injuries to MCL more prevalent than LCL • MCL • foot planted and force applied to the lateral side of knee • football
A noncontact mechanism was reported in 71 (72%) knees and a contact injury in 28 (28%) knees. Most of the injuries were sustained at footstrike with the knee close to full extension. Noncontact mechanisms were classified as sudden deceleration prior to a change of direction or landing motion, while contact injuries occurred as a result of valgus collapse of the knee.
NON-CONTACT INJURY The more common opposite non-contact injury occurs when the athlete plants the foot and rotates to the opposite side, such as illustrated by this badminton player.