Cholesterol Embolization Syndrome Mimicking Vasculitis: A Case of Lower Extremity Ulceration with Longstanding Seropos
Cholesterol Embolization Syndrome Mimicking Vasculitis: A Case of Lower Extremity Ulceration with Longstanding Seropositive Rheumatoid Arthritis. . Samar Charabaty, MD; Victoria Shanmugam, MBBS, MRCP.

Cholesterol Embolization Syndrome Mimicking Vasculitis: A Case of Lower Extremity Ulceration with Longstanding Seropos
E N D
Presentation Transcript
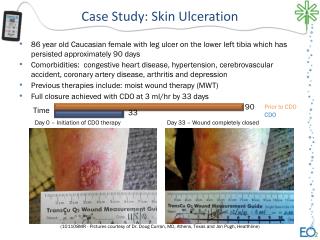
Cholesterol Embolization Syndrome Mimicking Vasculitis: A Case of Lower Extremity Ulceration with Longstanding Seropositive Rheumatoid Arthritis. Samar Charabaty,MD; Victoria Shanmugam, MBBS, MRCP. Department of Rheumatology, Allergy and Immunology, Georgetown University Medical Center, Washington DC. Georgetown University Abstract Hospital Course We present the case of a 65 - year- old caucasian man with coronary artery disease, peripheral vascular disease and rheumatoid arthritis who develops gangrene of the foot. In this presentation, we review causes of lower extremity ulceration associated with rheumatoid arthritis, and recognize cholesterol crystal embolization syndrome as a potential complication of atherosclerosis and mimicker of vasculitis. • HD 1 : right partial calcanectomy. • HD 4 : Total Below the knee amputation. • HD 10 : Patient developed pulmonary embolism and was started on anticoagulation. • HD 11 : The skin of the left foot took a mottled appearance. • HD 15 : An arteriogram of the lower extremity showed PVD and a moderate length near total occlusion of the superficial femoral artery ( figure 2). • HD 18 : A left femoro-popliteal bypass was done to re-establish flow to the left lower extremity. • HD 27 : right lower extremity amputation flap became gangrenous despite patent vasculature and no evidence of infection. The rheumatology team was asked to evaluate for vasculitic processes. Introduction • Cholesterol crystal embolization (blue toe syndrome) is a syndrome in which portions of atherosclerotic plaque embolize distally, occluding small arteries and causing tissue ischemia • Although this may can occur spontaneously, it is often associated with invasive vascular procedures such as arteriograms and vascular surgery. Figure 3: Skin biopsy specimen showing cholesterol clefts in a small arteriole (Hematoxylin & eosin stain). • Peripheral artery disease: • Atherosclerotic peripheral artery disease is more common in rheumatoid arthritis patients than healthy controls independent of other cardiovascular risk factors. • Inflammatory markers, glucocorticoid use and extra-articular features of rheumatoid arthritis are independent risk factors in this population. • Presence of biphasic pulses in the right foot at presentation, and intact blood flow to the amputation flap all suggested that some other factor may be playing a role in the progression to gangrene. • Cholesterol crystal embolism: • Biopsy demonstrating cholesterol “clefts” in the small or medium-sized arteries or arterioles. These crescentic or elongated ovoid spaces are the result of dissolution of the cholesterol crystal during tissue fixation and are pathognomic of cholesterol embolization syndrome. Learning Objectives 1-To review causes of lower extremities ulceration associated with rheumatoid arthritis. 2- To recognize cholesterol crystal embolization syndrome as a potential complication of atherosclerosis and a vasculitis mimicker. • A full autoimmune came back negative and the hypercoagulable work-up revealed an elevated of the homocysteine level at 13.5 umol/l (normal: 4.3-11.4), along with heterozygous plasminogen activator inhibitor-1 gene mutation (table 1). • The debrided tissue from the amputation site was reviewed in detail, and cholesterol clefts were identified in a small arteriole confirming the diagnosis of cholesterol crystal embolization syndrome (figure 3) • This patient commenced 20 mg of prednisone, with taper over the subsequent weeks. • LDL apheresis was considered, but deferred due to clinical stabilization. • Since the patient had prothrombotic risk factors and a recent pulmonary embolus, the anticoagulation was continued. No further ischemic events were noted, and patient was discharged to a rehabilitation facility. Case Presentation • A 65-year-old caucasian man with coronary artery disease and bypass surgery in 1995, peripheral vascular disease, dyslipidemia and heavy smoking, presented 4 months after starting adalimumab for longstanding seropositive erosive rheumatoid arthritis with a myocardial infarction. He was treated with endovascular stenting. Subsequently, he developed right foot pain and blue discoloration of his toe. His podiatrist treated his foot pain with a steroid injection for presumed plantar fascitis. He later developed progressive ulceration and gangrene of the right heel and was admitted at Georgetown for further evaluation. • He denied any systemic symptoms and his rheumatoid arthritis was stable with approximately one hour of morning stiffness in the hands and mild swelling in the metacarpophalangeal joints. • On the heel of the right foot, there was a gangrenous ulcer (figure 1), but dorsalis pedis and posterior tibialis pulses were biphasic. On the left foot there was a submetatarsal blister, dorsalis pedis pulse was monophasic and the posterior tibialis pulse was absent. There were no other skin rashes, livedo reticularis, splinter hemorrhages or Bywater’s lesions. Neurological examination was unremarkable. Discussion • Based on a prospective observational study of 1786 cardiac catheterizations, the rate of cholesterol embolization syndrome is estimated to be approximately 1.4 % (2). • Major risk factors for cholesterol emboli include advanced age, vascular procedures, and peripheral vascular disease. • The prognosis of CCE is poor with a 72% fatality rate due to concomitant visceral ischemia. • Some studies have implicated anticoagulation as a precipitant for CCE (3). However, in a study of 519 patients with severe aortic plaque the rate of cholesterol emboli was similar in those receiving warfarin as those who were not (1%) (4). • Treatment remains supportive. Statins, which stabilize and may cause regression of atherosclerotic plaques, improve renal and overall outcome. Additionally, steroids, iloprost and LDL apheresis have been beneficial in small numbers of patients. Differential diagnosis • Rheumatoid vasculitis: • Typically develops in patients with longstanding erosive disease. • Commonly involves small and medium-sized vessels of the skin, digits, peripheral nerves, eyes and heart. • Risk factors include male gender, high-titer rheumatoid factor, joint erosions, pleuritis, subcutaneous nodules, and presence of nail-fold lesions. • Vasculitis related to TNF-α inhibitor use: • Several reports suggest that TNF-α inhibitors induce vasculitis, others have reported a successful response of rheumatoid vasculitis to these drugs • Most vasculitis cases (86%) involved skin lesions including purpura, ulcerative lesions, nodules, digital vasculitis, maculopapular rash and chilblain lesions (1). Vasculitis appeared after a mean of 38 weeks of therapy and in most cases resolved with discontinuation. Adalimumab was implicated in only 4% of cases in this study, and there were no reports of cardiac involvement. • Prothrombotic states: • Both acquired and inherited hypercoagulable states should be suspected when unusual, migratory, or widespread locations of thrombosis are seen at early age of onset; with recurrent episodes; and a strong family history • Both heterozygous plasminogen activator inhibitor-1 mutation, and elevated homocysteine level may have contributed to the development of the pulmonary embolus but are not typically associated with arterial thrombi. Conclusion Cholesterol crystal embolism is a well recognized mimicker of vasculitis and should be considered in rheumatoid athritis patients presenting with tissue ischemia following a vascular procedure. References • Ramos-Casals M et al. Autoimmune diseases induced by TNF-targeted therapies. Best Pract Res Clin Rheumatol. 2008;22(5):847-61. • Bashore TM, Gehrig T. Cholesterol emboli after invasive cardiac procedures. J Am Coll Cardiol. 2003;42(2)::217-8. • Hyman BT et al. Warfarin-related purple toes syndrome and cholesterol microembolization. Am J Med. 1987;82(6) :1233-7. • Tunick PA, et al. Effect of treatment on the incidence of stroke and other emboli in 519 patients with severe thoracic aortic plaque. Am J Cardiol. 2002;90(12):1320-5. Figure 2: Arteriogram of the left lower extremity showing occlusion of the superficial femoral artery Figure1: Gangrenous ulcer on the heel of the right foot.