Multiple Sclerosis
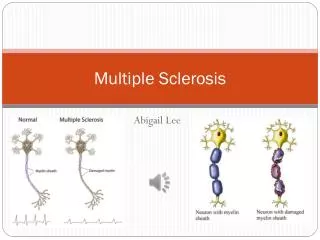
Multiple Sclerosis MS is a common case of chronic disability in young adults. Disease is characterised by episodes separated in time and space, in which areas of the central nervous system become demyelinated (plaques). These plaques often are centred around venules.


Multiple Sclerosis
E N D
Presentation Transcript
Multiple Sclerosis MS is a common case of chronic disability in young adults. Disease is characterised by episodes separated in time and space, in which areas of the central nervous system become demyelinated (plaques). These plaques often are centred around venules. Around half of all patients with the disease are unable to walk unaided within 15 years of diagnosis.
Q1 - How does MS present? (1) • General • MS typically presents in young adults , and usually follows a relapsing and remitting course • It is difficult to predict the prognosis of an individual patient, and it is important to recognise that some patients do not have the relapsing and remitting pattern of the disease • Occasional patients develop a rapidly progressive disease. These cases may even mimic tumours, and biopsies from these patients may be necessary, and can be very difficult to interpret accurately • At the other end of the clinical spectrum, some patients may have a remitting and relapsing form of the disease, with minimal residual disability between episodes of relapse • Some patients suffer a single episode of demyelination, and do not subsequently develop multiple sclerosis
Q1 - How does MS present? (2) • Signs and symptoms • A variety of these may occur depending on anatomical location of the plaques • Visual symptoms: • Optical neuritis (pain, blurred vision, impaired acuity, impaired colour vision, visual field defect, afferent papillary deficit) • Diplopia resulting from brainstem plaque • Sensorimotor disturbances: • Spastic paraparesis • Dysaethesthesiae • Pain in some patients (limbs or trigeminal distribution)
Q1- How does MS present? (3) • Other symptoms/signs • Increased incidence of epilepsy • Bladder disturbance • Erectile dysfunction • Lhermitte phenomenon (tingling shooting into limbs on neck flection) • Symptoms may be worse after a hot bath
Q2- What are the key clinical features and laboratory tests that aid diagnosis?(1) • Clinical features • The clinical features are central to the diagnosis. The distribution of lesions in time and space are characteristic of the disease • Diagnosis requires occurrence of at least two lesions in the central nervous system, separated in time and space • Signs and symptoms that may occur include: optic atrophy, cerebellar dysarthia, ataxia, urinary symptoms, spastic paraparesis, dementia, and mood disturbance
Q2- What are the key clinical features and laboratory tests that aid diagnosis?(2) • MRI of brain/spinal cord (plaques) • Visual evoked potential (delayed central conduction in the visual pathways) • Cerebrospinal fluid examination findings are non-specific: • Increased lymphocytes in active phase, raised protein. Oligoclonal bands on electrophoresis (local synthesis of immunoglobulins) • Any of these tests can produce false positives and false negatives
Plaque in the spine http://medlib.med.utah.edu/kw/ms/
Q2- What are the key clinical features and laboratory tests that aid diagnosis?(3) • Histological assessment is only occasionally necessary. This is usually in patients with atypical presentations. • Studies comparing the clinical, radiological and post-mortem neuropathological features of MS are continuing to provide insights into this disease
Q3- What are the mechanisms of pathogenesis leading to the symptoms seen? Severe demyelination prevents conduction of nerve impulses through myelinated axons; partial myelin injury results in delayed conduction, inability to transmit fast trains of impulses. • Autoimmune response - damage caused by inflammatory cells – T cellsandmacrophages. Structure of plaques. • Role of infectious agents – Circumstantial evidence • Induction of autoimmunity through mimicry?
Q3- What are the mechanisms of pathogenesis leading to the symptoms seen? Severe demyelination prevents conduction of nerve impulses through myelinated axons; partial myelin injury results in delayed conduction, inability to transmit fast trains of impulses.
Q3- What are the mechanisms of pathogenesis leading to the symptoms seen? Severe demyelination prevents conduction of nerve impulses through myelinated axons; partial myelin injury results in delayed conduction, inability to transmit fast trains of impulses. • Autoimmune response - damage caused by inflammatory cells – T cellsandmacrophages. Structure of plaques. No evidence for B cell autoreactivity
Pathogenesis of Multiple sclerosis • Evidence for T cell responses against myelin basic protein • Pathogenesis mediated mainly by T cells and macrophages
Q3- What are the mechanisms of pathogenesis leading to the symptoms seen? Severe demyelination prevents conduction of nerve impulses through myelinated axons; partial myelin injury results in delayed conduction, inability to transmit fast trains of impulses. • Autoimmune response - damage caused by inflammatory cells – T cellsandmacrophages. Structure of plaques. • Role of infectious agents – Circumstantial evidence
Q3- What are the mechanisms of pathogenesis leading to the symptoms seen? Severe demyelination prevents conduction of nerve impulses through myelinated axons; partial myelin injury results in delayed conduction, inability to transmit fast trains of impulses. • Autoimmune response - damage caused by inflammatory cells – T cellsandmacrophages. Structure of plaques. • Role of infectious agents – Circumstantial evidence • Induction of autoimmunity through mimicry?
Q4- What are the current treatments and how are they thought to work? (1) • Treatments that aim to modulate the immune system are being developed, but the indications for their use are still controversial. • Treatment with interferons is of benefit to some patients (but not curative), but have significant side effects in many patients – cost implications • Corticosteroids can be used to reduce the time to recovery in episodes of relapse
Q4- What are the current treatments and how are they thought to work? (2) • Treatments aimed at relieving symptoms can be important in improving the quality of life for some patients. Eg. baclofen and diazepam can reduce spasticity, and bladder symptoms can be treated with anticholinergic drugs. ? Cannabis? • Intermittent self-catheterisation may be useful in some patients with bladder dysfunction • Some patients benefit from care from a multidisciplinary neuro-rehabilitation team. Surgery is occasionally needed to ameliorate spasticity
Some references: CH Polman, BMJ Uitdehagg, BMJ 2000:321. 4904 Lecture notes in neurology 7th Edition. Blackwell Science. Lionel Ginsberg
For more information contact Professor D Katz - d.katz@ucl.ac.uk More information will be given to the students at the session on Intercalated courses for 2005