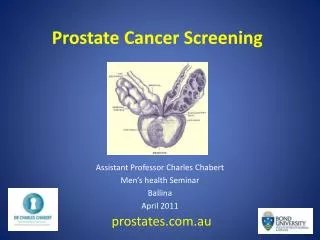
Prostate cancer screening
Prostate cancer screening. Dr J P McMenamin. Prostate cancer. An important health problem in NZ. Approx 500 men die of prostate cancer every year. 13% male cancer deaths (3 rd most common after lung and bowel). Prostate cancer. 75% new diagnoses 70+ years Estimated lifetime risk of:

Prostate cancer screening
E N D
Presentation Transcript
Prostate cancer screening Dr J P McMenamin
Prostate cancer • An important health problem in NZ. • Approx 500 men die of prostate cancer every year. • 13% male cancer deaths • (3rd most common after lung and bowel)
Prostate cancer • 75% new diagnoses 70+ years • Estimated lifetime risk of: diagnosis = about 16% prostate cancer death 3% to 4% • Most common in older men • Most men with prostate cancer survive
Current practice • Many NZ GPs are screening • Opinions and practice are mixed • Mostly opportunistic and selective • Mostly using DRE/PSA • Tendency to investigation of borderline abnormal results • Some medical opinions and Prostate Support Groups advocate screening
Major Risk factors • Age (45% over 70yrs, 30% over 80yrs) • Ethnicity (African American ethnicity a risk, Maori incidence rising) • Family history ( up to x 2 for one, x 5 – 11 for more affected 1st degree relatives)
Prostate cancer screening tests • DRE generally reported to perform poorly (PPV 6 – 30%) • TRUS generally considered a diagnostic test (PPV 5-9 %) • PSA considered most hopeful though unproven screening test • (PPV 28-35%)
Methods to improve PSA detection of prostate cancer • High levels of complexed PSA, low levels of percent free PSA (free/total) associated prostate cancer • May be of most help in “grey zone” ( PSA 4 – 10) • No definitive evidence of improved screening outcomes compared with total PSA levels
PSA density • PSA density defined as serum PSA divided by gland volume • No definitive evidence of benefit as screening test
PSA Velocity • Serial increases in PSA may be associated with prostate cancer • Value as screening test remains unclear
PSA cut-off values • Usual screening cut-off is 4.0ng/ml • Reducing cut-off improves detection rate (sensitivity) but results in more biopsies (reduces specificty) • Age adjustment remains unclear (lower cut-off younger men = more biopsies, higher cut-off older men = more cancers missed)
The case for screening: a partial perspective • screening detects prostate cancer in a significant number of asymptomatic men. • A high proportion of cancers detected by screening are clinically localized at the time of diagnosis (screening has been shown to shift cancer detection to earlier stage) • Clinical outcomes after surgery for localized prostate cancer are known to be better
Regional mortality reductions • PSA screening is associated with reduced mortality in a number of reports
The Case against Prostate Cancer Screening: the rest of the argument • Prostate cancer mortality rates declined relatively early after the initiation of widespread screening • it is unlikely that screening has as yet contributed in a major way to the decline • It is more likely that the mortality reduction is a consequence of better prostate cancer management or improved treatment modalities.
The Case against Prostate Cancer Screening: the rest of the argument Most deaths (over 60%) occur in men 75 years of age and older (a reduction in all-cause mortality, resulting in an actual increase in life expectancy, will be difficult to accomplish in this age group)
Natural history not well defined • The natural history of prostate cancer has not been well defined, and there is great variation in the aggressiveness of different tumours • bias toward screening detection of biologically indolent tumours, which are associated with a good prognosis, rather than detection of aggressive tumours with a poor prognosis.
Waiting for the evidence • No definitive evidence of a benefit from screening yet • No definitive evidence of a mortality benefit from intervention (RCT has shown reduction in disease-specific but not all-cause mortality)
To screen or not to screen PSA results in the detection of cancers at an early stage. Treatment of early stage cancers has better disease outcomes
To screen or not to screen But the fact that a cancer can be detected earlier in its natural history is no guarantee that benefit will follow Screening for prostate cancer can substantially impair the quality of life of those with detected and treated cancer, that would not otherwise have reduced life expectancy.
Post-screening complications • Biopsy complications (infection 1%, bleeding 50%) • 2 year post-prostatectomy - Some degree incontinence 38% - Sexual dysfunction 50% - 60%
Conclusion “Decisions on the introduction of population-based screening for prostate cancer cannot be made before RCTs have been completed.” The International Prostate Screening Trial Evaluation Group.
2 international RCTs • European Randomized Screening for Prostate Cancer • Prostate, Lung, Colorectal and Ovarian (PCLO) Cancer Screening Trial
Aiming for over 100,000 men in intervention and control arms • PSA + some DRE • 10% of screened men age 55-69 >4ng/ml so far -> 84% of these biopsied • Results 2005-2008
Conclusion • Evidence does not support active screening • Men requesting screening require information • Information needs to be up to date and readily available • NHC has published report and information resource