Download
1 / 55
560 likes | 763 Vues
Epidemiology of VTE in Patients with Cancer. Paolo Prandoni , MD, PhD University of Padua (Italy) ESMO, Stockholm 2008. 140. Ovary. 120. 117. 110. 120. Brain. 98. 100. Pancreas. 81. 76. 80. Lymphoma. Rate per 10,000 patients. 61. Leukaemia. 60. Colon. 40. Lung. 20. 0.

E N D
Epidemiology of VTE in Patients with Cancer Paolo Prandoni, MD, PhD University of Padua (Italy) ESMO, Stockholm 2008
140 Ovary 120 117 110 120 Brain 98 100 Pancreas 81 76 80 Lymphoma Rate per 10,000 patients 61 Leukaemia 60 Colon 40 Lung 20 0 Cancer type Risk of Thrombosis According to Cancer Type Adapted from Levitan et al, Medicine 1999.
Incidence Of VTE In Patient Hospitalized With Cancer Methods And Results • The number of patients discharged with a diagnostic code for 19 types of malignancies, pulmonary embolism or deep venous thrombosis from 1979 through 1999 was obtained from the National Hospital Discharge Survey. • In patients with any of the 19 malignancies studied, 827 000 of 40 787 000 (2.0%) had VTE, which was twice the incidence in patients without these malignancies, 6 854 000 of 662 309 000 (1.0 %).
Population-based, case-control study of 3220 patients with a first VTE episode and 2131 control individuals Adjusted OR of VTE in cancer patients: 6.7 (95% CI, 5.2-8.6) OR (95% CI) First 3 months after cancer diagnosis 53 fold increase Patients with distant metastases Higher Risk Cancer patients with thrombophilia Higher Risk The “MEGA” Study Adapted from Blom et al., JAMA 2005; 293:715-22.
Incidence of VTE Within 2 Years of Diagnosis of 5 Different Types of Cancer (235,149 cases) With metastatic disease With regional-stage disease Adapted from Chew et al, Arch Intern Med 2006.
Surgical procedures Prolonged immobilization (hospital stay) Chemotherapy Adjuvant hormonal therapy Administration of erythropoietin Central venous catheters Risk Factors Of Venous Thrombosis In Cancer Patients Adapted from: Bennett JAMA. 2008;299(8):914-924; Lyman JCO 2007;25 5490-5505.
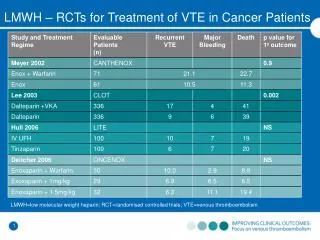
Kakkar, 1970 24/59 (41%) 38/144 (26%) Hills, 1972 8/16 (50%) 7/34 (21%) Walsh, 1974 16/45 (35%) 22/217 (10%) Rosenberg, 1975 28/66 (42%) 29/128 (23%) Pineo, 1979 10/30 (33%) 13/134 (10%) Allan, 1983 31/100 (31%) 21/100 (21%) Sasahara, 1984 9/37 (22%) 13/53 (24.5%) Sue-Ling, 1986 12/23 (52%) 16/62 (26%) TOTAL 138/376(37%)159/872(18%) Postoperative DVT in Cancer Patients Postoperative DVTCancer Non-cancer
Late Postoperative VTE in Cancer Patients OVERALL VTE PROXIMAL DVT PE ENOXACAN II Study, adapted from Bergqvist et al, 2002.
In Hospital Mortality Rate Due To Pulmonary Embolism in Immobilized Patients With and Without Cancer Mortality (%) 16 p=0.05 14 14 12 10 8 8 6 4 2 0 Non-cancer Cancer Adapted from Shen and Pollak, South Med J, 1980.
OR (95% CI) Previous VTE 2.06 (1.10-3.69) Acute infectious disease 1.74 (1.12-2.75) Cancer 1.62 (0.93-2.75) Age > 75 yrs 1.03 (1.00-1.06) Chronic respiratory disease 0.60 (0.38-0.92) Sub Analysis of the Medenox Study Adapted from Alikhan et al, Arch Int Med 2004.
OR (95% CI) Trauma < 3 months 7.9 (1.1-54.9) Platelet count > 350/nl 3.1 (1.4-7.0) Leg edema 3.0 (1.2-7.3) Cancer 2.8 (0.8-9.5) Pneumonia 2.7 (1.2-5.8) Predictors of VTE During Hospitalization in Medical Patients Adapted from Zakai et al, JTH 2004.
Weiss, 1981 433 Breast stage II 22 (5%) 0* Goodnough, 1984 159 Breast stage IV 24 (15%) 4 (2.5%) Levine, 1988 205 Breast stage II 14 (7%) 0* Saphner, 1991 2352 Breast 128(5%) 0* * statistically significant Venous and Arterial Thrombosis in Cancer Patients During Chemotherapy Type of Thrombosisn cancer during after chemotherapy
Development and Validation of a Predictive Model for Chemotherapy-associated Thrombosis Blood 2008 Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW
Risk Factors for Chemotherapy-associated VTE Low risk: score 0 Intermediate risk: score 1-2 High risk: score < 3 Adapted from Khorana et al. Blood 2008.
705 postmenopeusal women with breast cancer CMF regimen Total thromboembolic events 39 of 54 events occurred during chemotherapy Tamoxifen and Chemotherapy Rate of thrombosis (%) 16 p=0.0001 14 9.6% 12 10 8 6 1.4% 4 2 0 Tamoxifen Tamoxifen + CT (n=352) (n=353) Adapted from Pritchard et al., J Clin Onc, 1996.
Tamoxifen Alone Versus Placebo for Prevention of Breast Cancer: VTE Risk Tamoxifen Placebo DVT incidence (per year) 0.13 % 0.084 % PE incidence (year) 0.069% 0.023 % Adapted from Fisher et al., J Nat Cancer Inst, 1998.
Venous Thromboembolism And MortalityAssociated With Recombinant ErythropoietinAnd Darbepoetin Administration For TheTreatment Of Cancer-associated Anemia JAMA 2008; 299: 914-24 Bennett CL, Silver SM, Djulbegovic B, Samaras AT, Blau CA, Gleason KJ, Barnato SE, Elverman KM, et al.
Endpoint Total DVT Lokich, 1983 Venography 42% Bern, 1990 Venography 37% Monreal, 1996 Venography 61.7% Verso, 2005 Venography 18.0% Luciani, 2001 Doppler US 11.8% Couban, 2005 Clinical 4% Reichardt, 2002 Clinical 4% Karthaus, 2005 Clinical 3.4% Lee, 2006 Clinical 4.3% Incidence of CVC-related DVT without Prophylaxis
The Long-term Clinical Course Of Acute Deep Venous Thrombosis Prandoni P, Lensing AWA, Cogo A, Cuppini S, Villalta S, Carta M, Cattelan AM, Polistena P, Bernardi E, Prins MH Ann Intern Med 1996; 125:1-7.
Malignancy 58 (16.3%) Surgery (< 3 months) 68 (19.1%) Trauma or fracture 62 (17.5%) Thrombophilia 46 (13.0%) Immobilization (> 7 days) 52 (14.6%) Pregnancy or childbirth 7/161 (4.3%) Contraceptives 18/161 (11.2%) High dose estrogens 7 (2.0%) Prevalence of Potential risk factors for DVT (N=355) Adapted from Ann Intern Med 1996; 125:1-7.
Baseline features RR Malignancy (n=58, 16%) 1.72 Thrombophilia (n=46, 13%) 1.44 Recent surgery (n=68, 19%) 0.36 Trauma/fracture (n=62, 17%) 0.51 Risk factors for VTE Recurrences
Recurrent Venous Thromboembolism And Bleeding Complications During Anticoagulant Treatment In Patients With Cancer And Venous Thrombosis Blood 2002; 100: 3484-88 Prandoni P, Lensing AWA, Piccioli A, Bernardi E, Bagatella P, Simioni P, Girolami B, Marchiori A, Scudeller A, Sabbion P, Noventa F, Girolami A
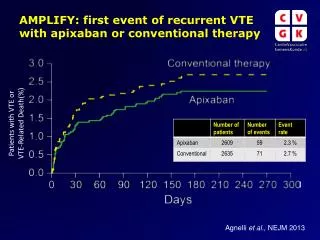
Cumulative Incidence Of Recurrent Thromboembolism In Patients On Anticoagulant Therapy % 20 cancer no cancer 18 Risk ratio=3.2; P<0.001 10 5 12 2 4 6 8 10 Months
CATEGORIES CANCER NON CANCER RR (95%CI) Severe (Stage IV) 54.1% 12.8% 4.6 (2.3-9.0) Mod. Severe (Stage III) 44.1% 12.8% 5.3 (2.5-10.9) Less severe (Stage I/II) 14.5% 12.8% 1.9 (0.8-4.2) Incidence of Recurrent VTE by Cancer Stage
Cumulative Incidence Of Major Bleeding On Anticoagulation Therapy 20 % cancer HR=2.1; P=0.019 no cancer 15 10 5 12 2 4 6 8 10 Months
CATEGORIES CANCER NON CANCER RR (95%CI) Severe (Stage IV) 42.8% 8.6% 4.8 (2.3-10.1) Mod. severe (Stage III) 19.1% 8.6% 2.5 (0.9-6.7) Less severe (Stage I/II) 3.4% 8.6% 0.5 (0.1-2.1) Incidence Of Major Bleeding By Cancer Stage On Anticoagulation Therapy
Predicting Recurrences Or Major Bleeding In Cancer Patients WithVenous ThromboembolismFindings From The RIETE Registry Thromb Haemost 2008; 100: 435-9 Trujillo-Santos J, Nieto JA, Tiberio G, Piccioli A, Di Micco P, Prandoni P, Monreal M
Main Clinical Characteristics Of Cancer Patients Who Did And Did Not Experience Recurrent VTE And Major Bleeding
Multivariate Analysis On The Risk To Develop Recurrent PE, Recurrent DVT, Or Major Bleeding
Aderka, 1986 9/35 (25.7) 2/48 (4.2) Monreal, 1988-91-97 8/148 (5.4) 4/718 (0.6) Prandoni, 1992 11/145 (7.6) 2/105 (1.9) Ahmed, 1996 3/113 (2.7) 0/83 (0) Hettiarachchi, 1997 10/155 (6.5) 3/171 (1.8) Rajan, 1988 13/152 (8.6) 8/112 (7.1) Subirà, 1999 0/10 (0) 0/30 (0) Schulman, 2000 93/534 (17.4) 18/320 (5.6) TOTAL 147/1292(11.4) 37/1587(2.3) Development of Subsequent Cancer Idiopathic VTE Secondary VTE
Sorensen et al, NEJM 1998;338:1169-73 Baron et al, Lancet 1998;351:1077-80 Murchison et al, Br J Cancer 2004;91:92-5 White et al, Arch Intern Med 2005;165:1782-87 Wide Population-based Studies
Sorensen, DVT 1737 1372 1.3(1.21-1.33) Sorensen, PE 730 556 1.3(1.22-1.41) Baron 2509 784 3.2(3.1-3.4) Murchison 4441 3469 1.3 (1.25-11.33) White 596 443 1.3 (1.2-1.5) Study Results Cancers Observed Expected SIR SIR = standardized incidence ratio
Risk of Cancer in Relation to Length of Time 4.0 DVT PE 3.0 SIR- Standardized incidence ratio 2.0 1.0 0-6 m 6-12 m 1-2 y 2-5 y 5-10 y > 10 y Adapted from Sorensen et al., NEJM 1998;338:1169-73.
Risk Of Cancer By Years After Hospital Admission 4.0 3.0 SIR- Standardized incidence ratio 2.0 1.0 0 2 4 6 8 10 12 14 16 18 20 22 24 Years after hospital admission Adapted from Baron et al., Lancet 1998;351:1077-80.
Increased Incidence Of Neoplasia Of The Digestive Tract In Men With Persistent Activation Of The Coagulant Pathway J Thromb Haemost 2004 Miller GJ, Bauer KA, Howarth DJ, Cooper JA, Humphries SE, Rosenberg RD
Population-based study 3052 middle-aged men, registered with 9 general practices in England and Scotland Annual measurement of prothrombin fragment 1+2 and fibrinopeptide A for 4 years Definition of persistent activation of the hemostatic pathway: increased values in two consecutive examinations Study Design Adapted from: Miller GJ, Bauer KA, Howarth DJ, Cooper JA, Humphries SE, Rosenberg R Increased Incidence Of Neoplasia Of The Digestive Tract In Men With Persistent Activation Of The Coagulant Pathway. J Thromb Haemost 2004 .
Total mortality (/1000 p-yrs) 17.1 9.7 Mortality from all cancers 11.3 5.1 Total digestive cancers 8.5 2.9 Fatal digestive cancers 6.3 1.9 Main Results Persist activation Control group n=111 n=2941 Adapted from: Miller GJ, Bauer KA, Howarth DJ, Cooper JA, Humphries SE, Rosenberg R Increased Incidence Of Neoplasia Of The Digestive Tract In Men With Persistent Activation Of The Coagulant Pathway. J Thromb Haemost 2004.
The Risk Of A Second Cancer After Hospitalisation For Venous Thromboembolism Br J Cancer 2005 Sorensen HT, Pedersen L, Mellemkjaer L, Johnsen SP, Skriver MV, Olsen JH, Baron JA
N Engl J Med 2000 Incidence Of Cancer After Prophylaxis With Warfarin Against Recurrent Venous Thromboembolism Schulman S, Lindmarker P, for the Duration of Anticoagulation Trial
Cumulative Probability of Newly Diagnosed Cancer Adapted from Schulman S, Lindmarker P, for the Duration of Anticoagulation Trial Incidence Of Cancer After Prophylaxis With Warfarin Against Recurrent Venous Thromboembolism. N Engl J Med 2000 .
Lancet Oncology 2007; 8: 395–402 Use Of Warfarin And Risk Of Urogenital Cancer: A Population-based, Nested Case-control Study Tagalakis V, Tamim H Blostein M, Collet JP, Hanley JA, Kahn SR
Incidence Rate Ratios for Prostate, Bladder and Kidney Cancer