Download
1 / 54
550 likes | 658 Vues
Dive into the intricate structures of the respiratory system, from the nose to the alveoli, and learn how it functions to provide oxygen to cells and remove carbon dioxide. Discover the role of key organs like the trachea, bronchi, and lungs in facilitating efficient gas exchange.

E N D
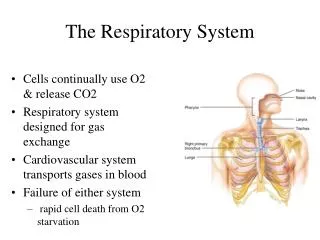
The Respiratory System • Cells continually use O2 & release CO2 • Respiratory system designed for gas exchange • Cardiovascular system transports gases in blood • Failure of either system • rapid cell death from O2 starvation
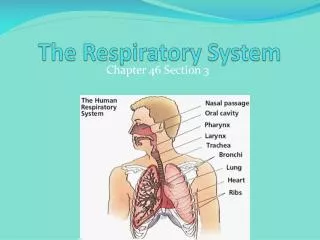
Nose -- Internal Structures • entrance – external nares • two nasal cavities with bony outgrowths = nasal conchae(superior, middle, inferior) • nasal cavities separated by nasal septum and nasal bone • superior most region of the cavity – site for olfactory epithelium - olfactory receptors for odors (smell) • lacrimal glands drain into nasal cavities • nasal cavities communicate with cranial sinuses (air-filled chambers within the skull) • nasal cavities empty into the nasopharynx - upper portion of the pharynx • connection between nasal cavity and nasopharnyx – internal nares • functions:warm, moisten, and filter incoming air
Nasopharynx From internal nares to soft palate Anatomical Landmark: openings of auditory (Eustachian) tubes from middle ear cavity adenoids or pharyngeal tonsil in roof Passageway for air only The Pharynx Oropharynx Laryngopharynx • From soft palate to epiglottis • Anatomical Landmark: behind the uvula • palatine tonsils found in side walls, lingual tonsil in tongue • Common passageway for food & air • Extends from epiglottis to cricoid cartilage • Anatomical Landmark: the epiglottis • Common passageway for food & air & ends as esophagus inferiorly
The Larynx • triangular box = “voicebox” • top of the larynx is a hole = glottis • covered with the epiglottis • contains the vocal cords - mucosal folds supported by elastic ligaments • Epiglottis---leaf-shaped piece of elastic cartilage • during swallowing, larynx moves upward bringing the glottis up to the epiglottis • epiglottis bends slightly to cover glottis • Laryngeal cartilages: • 1. thyroid cartilage (Adam’s apple) • 2. cricoid cartilage • 3. arytenoid cartilage – for the attachment of true vocal cords and arytenoideus muscles • filters, moistens, vocal production Tortora & Grabowski 9/e 2000 JWS
Vocal Cords • False vocal cords (ventricular folds) found above the true vocal cords • True vocal cords attach to arytenoid cartilages • True vocal cord contains both skeletal muscle and an elastic ligament (vocal ligament) • When intrinsic muscles of the larynx contract they move the artytenoid cartilages & stretch the true vocal cords tighter • When air is pushed past the tightened vocal ligament, sound is produced
Larnyx and Vocal Cords • true vocal cords vibrate upon passage of air -> speech • thickness determines frequency of vibration and timber of sound • thicker the cords – slower they vibrate – lower the pitch • thinner the cords – faster they vibrate – higher the pitch • thickness also controlled by testosterone • pitch can also be controlled by tightening the vocal cords voluntarily • tighter the cords – faster they will vibrate
Trachea • flexible cylindrical tube - Size is 5 in long & 1 in diameter • sits anterior (in front of) the esophagus • splits into right and left primary bronchi – enter the lungs • held open by “C” rings of hyaline cartilage = tracheal cartilage • 16 to 20 incomplete rings • open side facing esophagus contains smooth muscle = tracheal ligament • layers: • innermost layer (mucosa) = pseudostratified columnar with cilia & goblet cells • outer layer (submucosa) = loose connective tissue & mucous glands • functions:conducts air into the lungs, filtration, moistens mucosa submucosa
Trachea and Bronchial Tree • Primary bronchisupply each lung • Secondary bronchisupply each lobe of the lungs (3 right + 2 left) • Tertiary bronchisplits into successive sets of Intralobular bronchiolesthat supply each bronchopulmonary segment ( right = 10, left = 8) • IL bronchioles split into Terminal bronchioles-> these split into Respiratory Bronchioles • each RB splits into multiple Alveolar ducts which end in an Alveolar sac
Pleural Membranes & Pleural Cavity • Visceral pleuracovers lungs • Parietal pleuralines ribcage & covers upper surface of diaphragm • Pleural cavityis space between the two pleura • contains a small amount of fluid
Gross Anatomy of Lungs • Blood vessels & airways enter lungs at hilus • Forms root of lungs • Covered with pleura (parietal becomes visceral) • Base, apex (cupula), costal surface, cardiac notch • Oblique & horizontal fissure in right lung results in 3 lobes • Oblique fissure only in left lung produces 2 lobes
Alveoli • Respiratory bronchioles branch into multiple Alveolar ducts • Alveolar ducts end in a grape-like cluster = alveolar sac or lobule -each grape = alveolus
Alveoli • site of gas exchange by simple diffusion • from heart (right ventricle)-> Pulmonary artery multiple branches ending as the Pulmonary arteriole Capillary bed over Alveolus Pulmonary venule multiple veins Pulmonary vein heart (left atrium) • deoxygenated blood flows over the alveolus & picks up O2 via diffusion because the alveolar wall is very thin • Type I alveolar cells • simple squamous cells where gas exchange occurs • Type II alveolar cells (septal cells) • free surface has microvilli • secrete alveolar fluid containing surfactant • Alveolar dust cells • wandering macrophages remove debris
Respiration • internal respiration: cellular respiration • intracellular metabolic processes in the mitochondria which use O2 and produce CO2 • respiratory quotient (RQ) = ratio of CO2 produced to O2 consumed
Respiration • external respiration – exchange of O2 and CO2 between the external environment and the lungs • three steps: • 1. Ventilation • act of moving the air = ventilation or breathing • 2. Exchange • O2 and CO2 are exchanged between alveolar air and pulmonary blood • 3. Transport
Non –respiratory functions • 1. route for water loss and heat elimination • inhaled air is humidified and warmed before it is expired • 2. enhances venous return • respiratory pump – act of muscular contraction drives blood back to the heart • 3. maintains normal acid-base balance of the blood • removal of CO2 in expired air decreases the total amount of carbonic acid • 4. enables speech, singing and other vocalizations • 5. smell/olfaction • 6. removes, modifies, activates or inactivates materials passing through the pulmonary circulation
to understand external respiration – you need to understand the pleural membranes in relation to the lungs Tortora & Grabowski 9/e 2000 JWS
Respiratory pressures • air moves into the lungs because of a pressure gradients • three different pressures need to be considered: • 1. atmospheric (barometric) pressure • caused by the weight of air on objects on the Earth’s surface • 2. intra-alveolar (intrapulmonary) pressure • pressure within the alveolus • alveolus are directly connected to the outside through the respiratory tubes • therefore air moves due to a pressure gradient difference between IAP and AP Tortora & Grabowski 9/e 2000 JWS
Respiratory pressures • 3. intrapleural (intrathoracic) pressure • pressure within the pleural sac • at rest – subatmosperic pressure
Respiratory pressures • in breathing: • AP equilibrates with intra-alveolar pressure – this equilibration is what moves air in and out of the lungs • IP does not equilibrate with IAP or AP because there is no direct connection with the outer pleural cavity and the inside of the lungs or the atmosphere
Intrapleural fluid & TPG • the pleural cavity is larger than the unstretched lungs • but the lungs are stretched slightly to try and fill this cavity • HOW? • two forces stretch the lungs within the pleural cavity • 1. Transmural Pressure Gradient • 2. Intrapleural fluid cohesion Tortora & Grabowski 9/e 2000 JWS
Intrapleural fluid & TPG • 1. transmural pressure gradient (TPG) • intra-alveolar pressure always equilibrates with AP (760 mm Hg) and both pressure are greater than intra-pleural pressure (756 mm Hg) • net pressure difference = transmural pressure gradient • TPG is a pressure is pushing outward across the lung wall (from “ inside out”) and also a pressure pushing inward across the thoracic wall (air pushing in on the chest) • chest wall has a tendency to “spring” outwards – the TPG pushing in on the chest wall counteracts this and compresses the chest wall in • the lung has a tendency to collapse - the TPG pushing from within the lung outwards counteracts this force and keeps the lung inflated • because of this the lungs are slightly inflated within the thoracic cavity Tortora & Grabowski 9/e 2000 JWS
2. intrapleural fluid cohesiveness • thin layer of pleural fluid is found between the parietal and visceral pleural membranes • water molecules resist being pulled apart – results in cohesiveness in thin layers of water-based fluids • the cohesion between visceral and parietal pleura keeps the lungs slightly stretched • also plays are role in changing lung volume in breathing • as the thoracic wall expands – the parietal pleura is pulled along with the chest wall • this pulls the visceral pleura with it • expands the volume of the lungs Tortora & Grabowski 9/e 2000 JWS
TPG and the cohesiveness of the intrapleural fluid prevent the lungs and chest wall from separating • if the self-contained nature of the pleural cavities is disturbed (puncture) – air can rush in and equilibrate the intra-pleural pressure with atmospheric = pneumothorax • no transmural pressure gradient exists across the lung wall or the chest wall because AP, IAP and IP now equal Tortora & Grabowski 9/e 2000 JWS
Mechanism of Breathing: Boyle’s Law • flow of air in and out of the lung occurs due to cyclical changes in IAP relative to AP • IAP can be changed by altering the volume of the lungs • described in Boyle’s law • As the size of closed container decreases, pressure inside is increased • As the size of a closed container increases, pressure decreases
Mechanism of Breathing Inspiration: -at rest: pressure inside lung = pressure outside lungs (IAP=AP) -inhale - diaphragm contracts and drops, external intercostal muscles swing the ribcage up and out -increase in thoracic cavity volume results, increase in lung volume increases also -IAP drops = Boyle’s Law -air rushes in to equalize -muscles of inspiration do not act directly on the lungs but act to change the volume of the pleural cavities -due to the cohesiveness of intrapleural fluid – lung volume changes -increase in lung volume decreases the IAP directly
Mechanism of Breathing Expiration: occurs because of the elasticity of the lungs - PASSIVE -in addition: relaxation of diaphragm and intercostal muscles returns thoracic and pleural cavity volume to normal -IAP increases over AP- air leaves lungs to equalize
Mechanism of Breathing Expiration: -elasticity of the lung has two components: elastic recoil & compliance -elastic recoil – provided by the elastic nature of the connective tissue and the surface tension in the alveolus -alveolar surface tension: created by a thin film of fluid produced by the type I cells – coats the inside of the alveolus -the water molecules at an air-water interface are strongly attracted to one another = surface tension -the pressure of surface tension is directed inward alveolar collapse -therefore alveoli are coated with a surfactant to reduce surface tension -however, some surface tension still exists – this is what helps “deflate” the lungs
-compliance: how much effort is required to stretch or distend the lungs -i.e. how hard you have to work to blow up a balloon -compliance is a measure of how much the change in lung volume results from a given change in transmural pressure gradient -the less compliant a lung, the higher the TPG has to be to stretch the lung so it can expand enough to give a normal inspiration -increased TPG can only be accomplished by decreasing the intra-pleural pressure of the pleural cavity below its normal subatmospheric level – this requires greater expansion of the thorax and a more vigorous contraction of the inspiratory muscles -requires active inspiration and expiration – brings other muscles into play
Summary of Breathing • Alveolar pressure decreases & air rushes in • Alveolar pressure increases & air rushes out Tortora & Grabowski 9/e 2000 JWS
Forced expiration • abdominal mm force diaphragm up • internal intercostals depress ribs • Forced inspiration • sternocleidomastoid, scalenes & pectoralis minor lift chest upwards as you gasp for air
Airway resistance and air flow • amount of air moved into the lungs is not only determined by the pressure differences (IAP, AP) but by the resistance the air meets as it flows through the bronchial tubes • remember flow rate?? • F = ΔP/R • F = flow rate • ΔP = pressure gradient • R = resistance • primary determinant for airflow just like blood flow is vessel resistance
Bronchioles • surrounded by “ring” of bronchiolar smooth muscle that can control the diameter of the bronchiole smooth muscle
Airway resistance and air flow • normal individuals have large enough bronchial tubes so that negligible resistance is contributed • vessel diameter can be dramatically influenced by the contraction or relaxation of the smooth muscle layer found within the bronchial tubes • bronchodilation and bronchocontriction
Bronchiolar Smooth Muscle • sensitive to changes in local environment – specifically to CO2 levels • the flow of blood to the alveolus must be carefully balanced to match airflow • cardiac output to the alveolar capillaries can be controlled • by adjusting R of the blood vessels
Lung Volumes • normal breathing only requires 3% of total energy expenditure if compliance is kept high and surface tensions are minimized • during quiet breathing the lungs are only at 50% of their maximum capacity • measurement of lung volumes – using a spirometer
Respiratory Volumes and Capacities • tidal volume (TV) =amnt of air that enters or exits the lungs 500 ml per inhalation • inspiratory capacity (IC) = max. amnt of air taken in after a normal exhalation, 3500 ml • inspiratory reserve volume (IRV) = IC - TV, 3000 ml • residual volume (RV) =amnt of air left in lungs after forced expiration 1200 ml • expiratory reserve volume (ERV) = amnt of air forcefully exhaled, 1100 ml • functional residual capacity = ERV + RV,2300 ml • vital capacity = max. amnt of air capable of inhaling, IRV + TV + ERV = 4600 ml • total lung capacity = VC + RV Tortora & Grabowski 9/e 2000 JWS
Alveolar ventilation • changes in lung volume are one factor in the overall determination of pulmonary ventilation = amount of air breathed in and out in one minute • another factor is respiratory rate • Pulmonary ventilation = Tidal Volume x Respiratory rate (RR) • not all inspired air reaches the alveolus – part remains in the conducting airways = anatomical dead-space • greatly affects the efficiency of pulmonary ventilation • amount of atmospheric air exchanged between the atmosphere and the alveoli per minute= Alveolar Ventilation • AV = [TV-dead space] x RR
Internal Respiration: Gas Exchange & Dalton’s Law • Each gas in a mixture of gases exerts its own pressure • as if all other gases were not present • partial pressures denoted as p • Air = 21% O2, 79% N2 and .04% CO2 • Total pressure is sum of all partial pressures • atmospheric pressure (760 mm Hg) = pO2 + pCO2 + pN2 + pH2O • to determine partial pressure of O2-- multiply 760 by % of air that is O2 (21%) = 160 mm Hg
Gas Exchange 1. External Respiration: exchange between air and blood in the pulmonary circuit • blood plasma entering the pulmonary capillaries has a lower pO2 (40 mm Hg) than air in the alveoli (105 mm Hg) • oxygen diffuses into the plasma, then into the RBC -opposite it true for CO2 • blood entering the pulmonary capillaries has a higher pCO2 (45 mm Hg) than air in the alveoli (40 mm Hg) • therefore CO2 diffuses out of the blood into the air of alveoli 2. Internal respiration: • exchange of gases between the blood and tissues • diffusion of oxygen into tissues results because pO2 is lower in the tissues (40 mm Hg vs. 100 mm Hg in the blood plasma) Tortora & Grabowski 9/e 2000 JWS
Gas Exchange Tortora & Grabowski 9/e 2000 JWS
Other determinants of gas exchange • effect of surface area – during exercise, the surface are for exchange can be increased to enhance the rate of gas transfer • effect of thickness between blood plasma and air – according to Fick’s law, increase thickness of a membrane decreases diffusion rates • increase thickness of the exchange surface in the lung can occur through • 1. pulmonary edema • 2. pulmonary fibrosis • 3. pneumonia - accumulation of fluid due to inflammatory response
Other determinants of gas exchange • effect of diffusion coefficient – rate of gas transfer is proportional to a diffusion coefficient (D) • D is related to the solubility of the gas and its molecular weight • D for CO2 is 20 times that of O2 – CO2 is more soluble in body tissues and blood plasma • therefore rate of CO2 transfer is 20X that of O2 • offset by the partial pressure gradient for O2 which results in equal amounts of O2 and CO2 exchanged at the lungs
Gas transport: Hemoglobin • O2 as a molecule dissolves poorly in the plasma of blood • oxygen is carried in the blood by hemoglobin = oxyhemoglobin -this does not directly contribute to the pO2 of the blood -the pO2 of the blood is a measure of the dissolved O2 in the plasma – which is related to the pO2 in the inhaled air Tortora & Grabowski 9/e 2000 JWS
Gas transport: Hemoglobin • Hb has a definite binding capacity - affected by the amount of O2 dissolving in the blood • in the pulmonary capillaries over the alveolus - the concentration of O2 in the blood plasma (the pO2) increases – promotes the binding of O2 to Hb • in the systemic capillaries of the tissues – blood plasma pO2 decreases – reaction is driven the opposite direction to form Hb + O2
100 mmHg of pO2 in the blood plasma translates into 98% saturation of Hb • if blood plasma pO2 falls below 100 mmHg there is little change in the saturation level of Hb until you get to about 60 mm Hg (~90% saturation) • 40 mm Hg (~75% saturation) • plateau phase provides a margin of safety • generally 98% of the Hb in blood is saturated with oxygen in the capillaries of the lungs • 60-70% saturated in the capillaries of tissues at sea level Tortora & Grabowski 9/e 2000 JWS
saturation level can be affected bytemperature (increase temp, decrease saturation) • saturation level can be affected by atmospheric pressure (decrease pressure, decrease saturation) • saturation level can be affected by blood pH (decrease pH, decrease saturation) • saturation level can be affected by CO2 concentration/plasma pH (decrease pH, decrease saturation) • shift in the saturation curve of Hb to the right (decrease saturation) = Bohr Shift • HOWEVER – these shifts do not dramatically change Hb saturation!!! Tortora & Grabowski 9/e 2000 JWS
Significance of Hb • so pO2 is the dissolved amount of O2 in the blood – creates the pressure gradient that drives O2 exchange with the lungs and at the tissues • Hb is a storage depot for O2 • when the blood enters the pulmonary capillaries surrounding the alveolus – the pO2 is considerably lower than alveolar pO2 diffusion of O2 from the lungs into the blood • as diffusion takes place - blood pO2 increases temporarily – drives the loading onto the Hb • the plasma pO2 then drops down to its original level – allows more diffusion from alveolar air into blood plasma • so the Hb soaks up the diffusing O2 – allows more diffusion at the lungs!!!! • at the tissues – O2 released from the Hb and moves into the plasma – temporary increase in pO2 – drives the movement into the tissues • Hb plays an important role in the total quantity of O2 that the blood can pick up in the lungs and drop off at the tissues Tortora & Grabowski 9/e 2000 JWS
CO2 transport Body tissue CO2 transport from tissues CO2 produced Interstitial fluid CO2 • CO2 is carried by the blood in 3 ways: 1. 90% of the CO2 combines with water in the RBC to form carbonic acid which immediately dissociates into bicarbonate and H+ ions (binds to Hb) • catalyzed by the RBC enzyme called carbonic anhydrase 2. some CO2 can dissolve in the plasma as carbonic acid H+ and bicarbonate 3. CO2 can combine with hemoglobin to form carbaminohemoglobin • in the lungs – Hb releases the H+ ion – it combines with the HCO3- to reform carbonic acid • carbonic acid breaks up into H2O and CO2 • CO2 is also released by Hb • CO2 diffuses into the alveolar air and is breathed out Plasma within capillary CO2 Capillary wall CO2 H2O Hemoglobin (Hb) picks up CO2 and H+. Red blood cell H2CO3 Hb Carbonic acid H+ HCO3 Bicarbonate HCO3 To lungs CO2 transport to lungs HCO3 H+ HCO3 Hemoglobin releases CO2 and H+. Hb H2CO3 H2O CO2 CO2 CO2 CO2 Alveolar space in lung