Smallpox
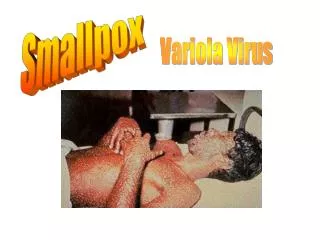
Smallpox. Jay Mung. Celia Rivera. Christopher Rinn. Introduction. Smallpox is a highly contagious human disease caused by the virus variola . Named from the Latin word varius meaning “spotted”. There are two strains:

Smallpox
E N D
Presentation Transcript
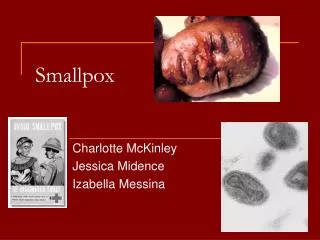
Smallpox Jay Mung Celia Rivera Christopher Rinn
Introduction • Smallpox is a highly contagious human disease caused by the virus variola. Named from the Latin word varius meaning “spotted”. • There are two strains: • Variola major, which has severe symptoms and a very high mortality (20-40%). • There are four types of variola major smallpox: • Ordinary (the most frequent type, accounting for 90% or more of cases); • Modified (mild and occurring in previously vaccinated persons); • Flat; And hemorrhagic (both rare and very severe). • Variola minor, which had less severe symptoms and lower mortality (about 1%). • It was named “smallpox” to differentiate it from the bubonic plague a.K.A. “Great pox”. • It wasn’t until the development of a smallpox vaccine, made from the closely-related vaccinia virus, that eradication was achieved.
History of Smallpox • It is thought that smallpox originated in Africa or china more than 3000 years ago. • From here it spread throughout the middle east. • There is evidence of a smallpox outbreak in Egypt around 1157BC. • The Egyptian pharaoh Ramses V’s mummy contains pock marks. • Linked to trade routes.
History of Smallpox • Smallpox reached Europe in 710 A.D. • Transferred to America in 1520 by Hernando Cortez’s assault on Techotitlan (Mexico City). 3.5 million Aztecs died in the following 2 years. • British colonists gave infected blankets to Native Americans during the French and Indian War. More than 50% of some tribes died. • 18th century European cities reached epidemic proportions.
History of Smallpox • Early eradication dates back to 1500 BC. The Turks induced a mild form of smallpox by pricking the skin of patients, inserting exudate from the postulates of the disease. Known as “variolation” • During the 10 century in the Szechuan region of China, Taoist alchemists exposed themselves to smallpox by inhaling the scabs of those with a mild infection. This was known as “insufflation”.
History of Smallpox • Because of the devastation caused by the disease, healers and physicians focused attention on it and its prevention. • The first step in prevention and treatment is understanding the nature of the disease. • Around 910 AD the Islamic physician Rhazes differentiated between smallpox and measles, which may seem similar at the onset. • Rhazes believed that once the disease passed, the individual would be immune to further diseases as the condition would not reoccur.
History of Smallpox • General George Washington used forced variolation to stop the spread of smallpox in his troops. • Washington was immune because he survived smallpox in Barbados in 1751. • However, a smallpox epidemic had reduced his healthy troop strength to half while the British troops, who had been variolated, were already immune to the spreading contagion. • Washington proclaimed smallpox to be his "most dangerous enemy"; and, by 1777 he had all his soldiers variolated before beginning new military operations.
History of Smallpox • During a smallpox epidemic in Gloucestershire, England in 1788 Edward Jenner made an interesting observation. • Milkmaids who worked with cattle and contracted the milder cowpox virus never contracted smallpox. • In 1796 Jenner inoculated 8 year old James Phipps with fluid from the lesion of milkmaid Sarah Nelmes. • James Phipps complained for several days of discomfort around his armpit; On the ninth day he felt chills and a headache. He soon fully recovered. • 6 weeks later, Phipps proved to be protected from the virus when Jenner exposed him to it.
Vaccine Discovered • To avoid confusion, inoculation with smallpox (as practised in Turkey) was termed "variolation" from "variola", the clinical term for smallpox. • Inoculation with cowpox (as practiced by Jenner) was termed "vaccination" from "vaccinia". • Initially, material for vaccination was obtained from genuine cowpox, by extracting liquid from the sores of someone with cowpox and inoculating this into a patient (as Jenner had done). • Arm-to-arm vaccination, with pustules taken from someone vaccinated a week earlier and inoculated into others (as also practised by Jenner), followed and became the form of immunisation in Britain. • By 1803 worldwide cowpox vaccination began . • Variolation of a healthy person was banned in Britain in 1840, under the terms of the Vaccination Act, which also meant anyone who gave another smallpox was liable to a month`s imprisonment.
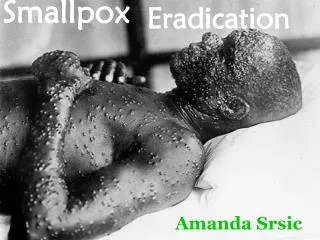
Smallpox Eradication • Throughout the nineteenth century smallpox vaccination was inconsistent at best. • In 1869, Chicago`s Board of Health made vaccination a requirement for children - but in 1872, there were 2,382 cases of smallpox with 655 deaths in the city. • In 1902, the Chicago Health Department developed a "vaccination creed", which promoted the supposed "benefits" of vaccination, stating, `true vaccination repeated until it "no longer takes" always prevents smallpox. Nothing else does`. This "creed" was taken up by the US military. • Nationally, there were 21,064 cases with 894 deaths in 1900. Annual averages for 1900-04 were 48,164 cases with 1,528 deaths. • In 1921, the number of cases had climbed to 102,791. • The last documented case of smallpox in the US was in 1949. • Sixty percent of the world’s population was still threatened by this disease when, in 1967, the world health organization (WHO) launched an intensive plan to eradicate smallpox. • It took a decade of intense international vaccination efforts, but the last natural case of smallpox occurred in Somalia in 1977. • A year later, a laboratory worker in the United Kingdom became infected while working with the vaccine.
Smallpox Eradicated • No other cases of smallpox have since been seen. • In May 1980, the World Health Organisation declared the global eradication of smallpox and recommended that all countries cease vaccination. • In 1986, the WHO first suggested all stocks of smallpox viruses should be destroyed. • For years, the US and Russia proposed - to sequence the virus - and the smallpox virus was given a "reprieve" until December 1993. • In May 1993, the WHO`s committee, which represented 156 nations, could not justify keeping the virus, and the committee`s recommendation to destroy the virus was endorsed by several groups including the American Society for Microbiology and the Council. • A small minority of American scientists expressed reservations. The deadline was postponed.
Destruction of Variola Virus stocks? • In September 1994, the ten-member WHO Ad Hoc Committee on Orthopox Virus Infections met, and unanimously agreed the potential cost to humanity from biological warfare or inadvertent outbreaks of the disease outweighed its supposed "benefits" to researchers. • To the WHO Committee, the most compelling argument to get rid of the smallpox strains was the potential for the virus to be used by terrorists for biological warfare. • Again, the decision to destroy the virus was tabled. • Rescheduling of the “deadline” took place in 1995 and again in 1999. • After resistance from the US and Russia, the deadline was extended yet again - this time to be "not later than 2002". • Finally, in January 2002, the United Nation`s health agency`s 32-member executive board met and endorsed a recommendation by the WHO`s Director General, Gro Harlem Brundtland, to drop the 2002 deadline and to set no new target for the destruction of the stocks of smallpox virus. • The world awaits the consequences........
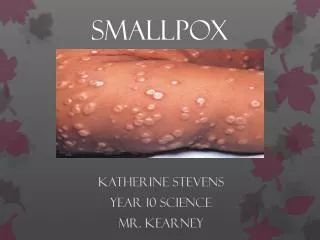
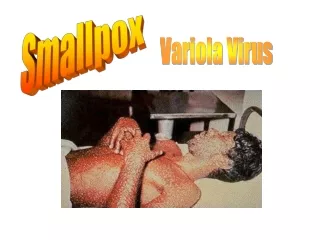
Smallpox was a fearful and devastating disease. If it didn't kill its victims, it scarred and disfigured them for life. Victim
Molecular Bio • Poxvirion is the largest of all virions. • Poxviruses replicate in cytoplasm rather than in nucleus • require various enzymes not found in DNA viruses • viral DNA-dependent RNA polymerase
Classification via RE Causative agents traditionally classified by signs and symptoms Situation changed by discovery of Muller et al (1978)
Features of Viral DNA • Single linear molecule • Largest of all viral genomes • Most DNA in genome unique • Virulence genes near termini/more variable • Genes for replication in central region of genome, highly conserved • Sister strands form single stranded circular molecule when denatured
Reactivation Non-genetic reactivation of “killed virus” Berry & Dedrick (1936) “killed virus” + non-virulent live-virus infection. Not to be confused with bacterial transformation:
Naked vs. enveloped Virions naturally released from cell are enclosed in envelope Virions released by cellular disruption are without envelope
Viral Replication I Adsorption and penetration of host cells • Enveloped virions • AKA Externally enveloped (EEV) • adsorbed more efficiently via endocytosis • Most virulent / easily spread • Naked virions • AKA intracellular mature virus (IMV) • outer membrane fuses with plasma membrane at cell surface • Naked virions used for vaccines
Viral Replication II • nucleoprotein core complex passes out of the virion • transcription system is produced • Virion formation • crescent/cupules w/ bilayer membrane and spicules form • more proteins produced for mature virion • DNA replication outside of nucleus
Viral Replication III • Most mature progeny virions remain cell-associated • released when cell undergoes necrosis • released from intact cells via budding • infects contiguous cells.
Changes on Cellular Level I • 1st –2nd hours noticeable toxic changes occur in cells • 4th hour viral factories appear in cytoplasm, • 16th hour aggregation of cells into hyperplastic foci / rupture
Changes on Cellular Level II ectodermal cells of chick embryo skin of patient with hemorrhagic smallpox
Proteins for Replication I • RAP94 • RNA-polymerase associated protein • confers specificity for early promoters • (shortens viral genome RNA polymerase ) • poly-A polymerase • Capping enzyme • topoisomerase • to early transcription factor
Proteins for Replication II • encoded by orthopoxviruses: • DNA polymerase • nucleoside triphosphatase • DNA glycosylase • thymidine kinase • thymidylate kinase • ribonucleotide reductase • dUTPase • Ribonuceoside reductase • small catalytic and a large regulatory unit • converts ribonucleoside diphosphates (NDPs) to deoxyribonucleoside diphosphates (dNDPs). • 70-80% structural homology with their eukaryotic counterparts
Proteins for Entering Cell • A33R, A34R, and A36R. • Mediates formation of the actin-composed microvilli • actin tails responsible for CEV’s efficiency in spread • allow CEV to be targeted to neighboring cells • CEVs mediate efficient cell-cell spread between neighboring cells • (whereas EEVs mediate long range transmission) • haemagglutinin and envelope glycoprotiens • Antigens promote cell fusion cell-to-cell spread of virions.
Proteins for Evading Host Immune Response I • Variola produces defense proteins: protection from host immune system • Virokines • resemble cytokines, secreted immune response regulatory proteins • secreted by infected cells • Viroreceptors • cellular receptors altered by virus • lose membrane anchoring sequences • bind ligands to form free-floating complexes in extracellular fluid • intracellular proteins • interfere with host’s normal signaling and enzymatic pathways.
Proteins for Evading Host Immune Response II • SmallPox Inhibitor of Complement Enzymes – (SPICE) • complement system destroys pathogens • viruses • virus-infected cells • SPICE prevents assembly of C3/C5 mediate immune response, by inactivating complement components • creates environment around variola-infected cells protected from complement-attack viral replication factories. • located in the terminal region of the variola genome.
Why is smallpox so lethal in Humans? • DNA replication begins one to two hours after infection • results in 10,000 copies of genome per cell • Half are packed into virions for further rounds of infection upon cell lysis. • Variola virus • uniquely suited to evading the human immune response • Whereas, Vaccinia • causes no disease in non-immunocompromised individuals • structural similarities cause it to be a good vaccine • produce antibodies specific to vaccinia and variola virulence factors.
Why is smallpox so dangerous? • Smallpox is a Category A bioterrorist threat. • It is extremely infectious: • The infective dose is only a few virions, which can be transmitted from the mouth of an infected person that is simply speaking or coughing. • Virus causes a painful and disfiguring illness. • Smallpox has a very high mortality rate of around 30%. • There is no specific treatment available.
Pathogenesis and Symptoms I Initial Symptoms/ Prodrome Phase (Duration: 2 to 4 days) • Infection occurs after the implantation of the virus onto the oropharyngeal or respiratory mucosa. After the virus begins to multiply in the local lymph nodes an asymptomatic viremia develops on the 3rd or 4th day. This is followed by multiplication of the virus in the bone marrow, spleen and lymph nodes. • The first symptoms include fever, head aches, malaise, and sometimes vomiting. High fevers occur in the range of 101 to 104 degrees Fahrenheit. At this time people are usually too sick to carry on their normal activities. Early Rash (Duration: ~4 days) • When the second viremia begins, the virus which was contained in leukocytes, localizes in small blood vessels of the dermis and beneath the oral and pharyngeal mucosa. This causes subsequent infection of the adjacent cells. • A rash first appears in the mouth and pharynx. These lesions ulcerate quickly releasing large amounts of the virus into the saliva. Patients are most contagious during the first week because the virus titers in the saliva are high.
Pathogenesis and Symptoms II • Soon after the sores arise in the mouth, the rash appears on this skin, beginning with the face and spreading to the arms, legs, hands and feet. The rash usually spreads to all parts of the body within 24 hours. As the rash appears, the fever usually subsides. • By the 4th day of the rash, the bumps are raised and filled with a thick, opaque fluid with a depression in the middle. Fever may begin to rise again until scabs form. Pustular Rash (Duration ~5 days) • The bumps become pustules, which are characteristically round, tense and deeply embedded in the dermis. Pustules and Scabs (Duration ~5 days) • By the end of the second week after the rash appears, most of the pustules have scabbed over. Resolving Scabs (Duration ~6 days) • The scabs fall off and characteristic pitted scarring gradually develops. The scars are most apparent on the face as a result of the destruction of sebaceous glands followed by shrinking of granulation tissue and fibrosis. • Individual is contagious to others until all of the scabs have fallen off.
Pathogenesis and Symptoms III Quote from P. Tiessier, Academy of Medicine in France, January 23, 1923. “As the result of intensive inflammatory swelling, the festinum becomes hideous, with bulging face and bright red cheeks, swollen and closed eyelids, turned-out lips, with fungal infection (where the edges of the lips become swollen and bleed easily) and bleeding. From the half open mouth a dribble of saliva constantly and abundantly runs and is fetid; with blocked nasal passages a pussy liquid oozes (purulent and bloody) and equally fetid; the tongue is swollen and ulcerous, the pharynx is covered with ulcers, which means that every effort to swallow gives rise to great pain. The poor patient whose body is covered in pus and gangrenous lesions in places, from which a nauseous and repugnant odour emanates, still suffers from an agonizing dyspepsia, from an unquenchable thirst, and from complete insomnia.”
Pathogenesis and Symptoms IV At least 90% of all smallpox cases are clinically characteristic and easily diagnosed. There are two forms of smallpox which are difficult to recognize: Hemorrhagic and Malignant. Hemorrhagic • Cases are uniformly fatal and occur among all ages and sexes, but pregnant women appear to be more susceptible. The incubation period is shorter and is characterized by severely prostrating prodromal illness: high fever, head, back, and abdominal pain. Erythema develops, followed by hemorrhages into the skin and mucous membranes. Death usually occurs by the 5th or 6th day after onset of the rash. Malignant • The sudden onset and prostrating prodromal symptoms are similar to the Hemorrhagic cases. Lesions develop slowly, but never progress to the pustular stage. Instead they remain soft, flat and velvety. This form is usually fatal, but if the patient does survive, the lesions usually disappear without forming scabs, or in more severe cases, large amounts of epidermis might peel off.
Transmission • Generally, direct and relatively prolonged face-to-face contact is required to spread smallpox from one person to another. • Smallpox can also be spread through direct contact with infected body fluids or contaminated objects (i.e. clothing and bedding). • Patients spread smallpox, mainly to family members and friends.