EMERGENCY DELIVERY
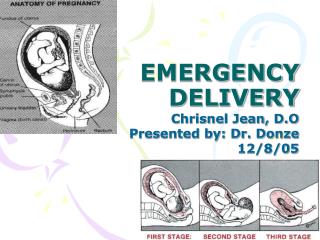
EMERGENCY DELIVERY. Chrisnel Jean, D.O Presented by: Dr. Donze 12/8/05. Evaluation of Pregnant Pt. Initially, ED physicians must determine the condition of the mother and the fetus in any pregnant women that present beyond 20 wks gestation. Evaluation of Pregnant Pt.

EMERGENCY DELIVERY
E N D
Presentation Transcript
EMERGENCY DELIVERY Chrisnel Jean, D.O Presented by: Dr. Donze 12/8/05
Evaluation of Pregnant Pt Initially, ED physicians must determine the condition of the mother and the fetus in any pregnant women that present beyond 20 wks gestation.
Evaluation of Pregnant Pt • Must consider obtaining the following info: • Medical history / Social history (drug use) • Obstetrical history • Parity (G0P1) • Gestational age (GA) – can be determined by the following: • LMP (Pregnancy wheel) • Fundal height (cm = wks of GA +/- 2 wks) Falsely elevated in obese pts • Ultrasound – detect congenital disorder / not an accurate predictor of GA in 3rd trim (varies +/- 3 wks) • EDC can be determined by: • Pregnancy wheel or Naegle rule = LMP+9months and 7days
Evaluation of Pregnant Pt Other Obstetrical history: • Prenatal care / OBGYN – Midwives • PNV • Complications from this recent and past pregnancy (Infection / Eclampsia / HELLP)
False Labor: Uterine contractions that do not lead to cervical changes Irregular (intensity / duration) confine to low ABD Known as Braxton-Hicks Tx with hydration / rest True Labor: Painful repetitive uterine contractions increase steadily in intensity and duration leads to progressive effacement and cervical dilatation Begins in fundus then radiate to pelvis. leads to progressive descent of fetus into pelvis. TRUE vs FALSE LABOR
Stage I Onset regular contraction to full cervical dilatation 2 phases: Latent / active (3 – 5 cm) Stage II Full dilatation to delivery Stage III Delivery infant to delivery placenta STAGES OF LABOR
PHYSICAL EXAMINATION • If pt present with no bleeding then do sterile speculum and bimanual exam. (Lubricant false nitrazine test if no PROM ) • Perform Ultrasound Prior to PE if pt present with bleeding to r/o placenta previa.
PHYSICAL EXAMINATION • Should include the following: • Inspect / palpate ABD for fundal hgt. • Cervix exam: • Effacement – thinning of the cervix (labor) • Dilatation – diameter of the internal cervical os (indicates progression of labor)
Station – the level that the fetus occupies in the pelvis with the reference point being the maternal ischial spine (palpable 4 and 8 o’clock in the vaginal canal) PHYSICAL EXAMINATION
PHYSICAL EXAMINATION • During PE of the pregnant pt, you should attempt to determine the presentation of the child (potential breech presentation or cord prolapse.) This can be done by the following method: • Leopold maneuvers • Digital examination
PHYSICAL EXAMINATION • Leopold Maneuvers: • Palpation of the fetus through the maternal abd to determine fetus position and presentation. • Used for screening for malpresenation / fetal weight. (sensitivity 28 – 88% / spec 94%)
PHYSICAL EXAMINATION 2.Digital examination: vertex presentation is best confirmed with palpation of the cranial sutures. Palpation of feet / hands malpresentation Note: verification of presentation is preferred by US
Spont. Rupture of Membrane • During the PE of pregnant pt you must evaluate for SROM • SROM determines and predicts imminence of labor and potential for complications • ”gush of clear or blood-tinged fluid” • The amount of fluid can be increase by Valsalva / standing. • SROM occur most commonly during active labor. Approx. 10% of 3rd trim will have SROM prior to labor
Confirmation of Spont. Rupture of Membrane • The presence of Amniotic fluid (SROM) can be confirmed by the following: • Nitrazine test: • Turns from yellow to dark blue in presence of Amniotic fluid (Amniotic pH=7 – 7.4) • Remain yellow color in presence of norm vaginal fluid (Vaginal pH = 4.5 – 5.5) • False positive can occur secondary to presence of blood, lubricant, Trich, seman, or cervical mucus.
2. Ferning /Microscopy NaCl crystals on a slide as amniotic fluid dries. Confirmation of Spont. Rupture of Membrane
Spont. Rupture of Membrane • PE must include evaluation for possible infection and presence of meconium: • Signs of chorioamnionitis • Maternal fever • Fetal tachycardia • Fundal tenderness • If membranes intact NO amniotomy in ED. Can lead to: • Precipitous labor • Cord prolapse
PROM: Premature Rupture of Membranes • PROM: • Rupture of amnion and chorion 1 hour or more prior to onset of labor. • PPROM (Preterm PROM): • Rupture occurs prior to 37 wks gestation. • Prolong ROM: • Occurs if delivery does not occur within 18 h of ROM.
PROM / PPROM • Possible causative factors include: • Infection • h/o PPROM • h/o trauma • Multiple gestations • Fetal anomalies • Placental abruption • Placenta previa
PROM / PPROM • OBGYN may use conservative management in <34 wks gestation. • More aggressive if: • Signs of chorioamnionitis/fetal distress • Maternal transport required - tocolytics • Delayed delivery to initiate steroids for lung maturation • Noninfectious PPROM may be prolonged with antibiotics • Erythromycin and ampicillin
Indicators Decel in FHR, persistent drop in FHR during contraction (lasting >30sec) Continue Fetal heart monitoring Doppler heart sounds - decelerations, episodic bradycardia >5min needs emergent C-sec Fetal Distress
Fetal Distress • Interventions: • Increase maternal blood flow • Increase maternal serum O2 conc. • Maternal positioning (L/R lateral, knee/chest) • Fetal scalp stimulation • Terbutaline Injections (stop contract/ incr. Blood Flow)
Emergency Delivery • Initial Step: • Obtain maternal VS, FHR • Initiate supportive tx • Venous access, maternal and fetal monitoring • Before transferring pt consider stage of labor / pt’s parity
Sterile Pelvic exam (Degree cervical dilatation/effacement, crowning, √ for fetus in introitus) Determine presenting part/position Palpate for skull sutures / fontanel, buttock, or extremity Emergency Delivery
Six Cardinal Movements: Engagement Flexion Descent Internal Rotation Extension External Rotation Process of Labor and Delivery
1-3 Perineum stretching /thinning allow passage of newborn Attempt to avoid Episiotomy 3-4 Control of fetal head to prevent large perineal tear and head / facial trauma to the newborn 4 Nose/mouth suctioning meconium? 4 Palpate neck for nuchal cord 4-6 Gentle traction avoid brachial plexus injuries (No jerky or forceful moves) Delivery Steps
6-7 “Slippery infant” 9-11 Double clamp umbilical chord and cut 12 Wrap/dry/gentle stimulation 12 Determine APGAR at 1 / 5 min. 12 Initiate neonatal resuscitation if a cyanotic / apneic child is delivered with no response to stimulation. Delivery Steps
Sign 0 points 1 point 2 points A Activity Absent Arms and legs flexed Active movement P Pulse Absent Below 100beats/min Above 100 beats/min G Grimace No response Grimace Sneeze,cough,pulls away A Appearance Blue-gray, pale all over Normal except for extremities Normal over entire body R Respiration Absent Slow, Irregular Good, crying APGAR
Delivery of Placenta • Occurs in 15-20m after infant is delivered • Allow spontaneous separation with gentle traction. • Aggressive traction on the cord can lead to: • Uterine inversion • Cord Tearing • Placenta disruption severe vaginal bleed
Delivery of Placenta • Massage uterus after delivery of placenta (promote contraction) • Oxytocin maintain uterine contraction (10–20u IV in 1 L NS at 250mL/h or 10u IM) • Uterine atony excessive vaginal bleed • Oxytocin, Methylergonovine or carboprost tromethamine • Delay episiotomy or laceration repair for OBGYN to perform.
In Cord Prolapse: Bimanual reveals palpable pulsating cord Elevate fetal part reduce cord compression Examiners hand should Remain in Vagina Transport Surgery C-sec is indicated. Do not attempt to reduce prolapsed cord Complications of Delivery: 1.Cord Prolapse
Complications of Delivery: 2. Shoulder Dystocia • Impaction fetal shoulder on pelvic outlet • Anterior shoulder trapped behind pubic symphysis • More common with large infant • Increased Morbidity / Mortality
Complications can include: Brachial plexus injury (overaggressive traction) Impaired respiration fetal hypoxia Cord compression compromised fetal circulation Complications of Delivery: 2. Shoulder Dystocia
Complications of Delivery: 2. Shoulder Dystocia • Downward traction will be insufficient to the deliver the anterior shoulder • Turtle sign – after delivering the infant’s head, it retracts tightly against the perineum • MacRoberts maneuver – position the mother in the extreme lithotomy position (legs sharply flexed up to the abd)
Complications of Delivery: 2. Shoulder Dystocia • Drain bladder/Consider episiotomy • Should apply suprapubic pressure to disimpact the ant. shoulder from the pubic symphysis. • NEVER APPLY FUNDAL PRESSURE further impact the shoulder on the pelvic rim. • Attempt delivery of posterior shoulder first
To deliver the impacted anterior Shoulder, a corkscrew maneuver should be attempted first. Grasps the posterior Scapula of the infants with 2 fingers and rotate the shoulder girdle 180 degrees in the pelvic outlet This rotate the post shoulder into the anterior position Woods’ maneuver
Complications of Delivery: 3. Breech presentation • Occurs in 3-4% pregnancies • 3 - 4 times higher morbidity • More common with prematurity • Head entrapment may occur secondary to incompletely dilated cervix. (normal cephalic delivery – the larger head dilates the cervical canal)
Associated with greater incidence of Fetal distress and cord entrapment Classified as the following Frank Complete Incomplete footling Complications of Delivery: 3. Breech presentation
Complications of Delivery: 3. Breech presentation Factors to remember: • Hands off let delivery occur spontaneously until umbilicus appears • Lateral force on medial thighs • Rotate fetus sacrum anterior position • Wrap exposed parts in towel • Follow the right humerus down • Turn fetus counterclock wise keep head in flexed position to deliver left arm • No traction risk head / arm entrapment • Footling and incomplete breach not safe for vaginal delivery cord prolapse / incomplete dilation of the cervix. • In any breech delivery consult OBGYN immediately.
Complications of Delivery: 4. Preterm Delivery • Preterm delivery • Most common precipitous childbirth • Common cause for emergency delivery • Gestational age may not be known • More often in breech position • Increased morbid and mortality • Control the delivery to reduce trauma to fragile preterm infant • More likely to require resuscitation
??Questions?? • Placenta previa rarely causes bleeding before the 3rd trimester. Any patient with vaginal bleeding in the 3rd trimester, especially if painless, should be presumed to have a previa until it is ruled out by __. A. bimanual examination with sterile gloves B. CT scan C. x-ray D. ultrasound
??Questions?? 2. Treatment for fetal bradycardia (<120) during labor includes all of the following except: • Maternal O2 and IV fluids to improve fetal oxygenation and placental perfusion. • Use maternal lateral positioning to relieve pressure on the inferior vena cava, improving venous return and placental perfusion. • For tetanic uterine contractions associated with fetal bradycardia in the absence of rapid progression of labor, terbutaline, 2.5 mg SQ may be used to relax the uterus. • Encourage more prolonged pushing to hasten delivery. • Consider uterine rupture, particularly if contractions seem to stop. • Consider cord prolapse and placental abruption as possible causes of fetal bradycardia.
??Questions?? • All of the following are true regarding abruptio placentae except: • Clinical findings include painful third trimester vaginal bleeding, with a tense, tender uterus. • Delivery is indicated (vaginal or c-section) for severe bleeding, maternal or fetal instability or abnormal coagulation studies. • Risk factors include previous abruption, smoking, hypertension, multiparity, trauma. • Shock can be reliably predicted from the amount of external bleeding. • Maintain volume and Hct; monitor mother and fetus; type & cross-match.
??Questions?? • Contraindications to the inter-hospital transfer of the gravida in labor include all of the following except: • Probability of delivery in transit. The acceptable amount of cervical dilation varies depending upon the circumstances, but in general a patient who is dilated >4-5 cm should not be transported. • Positive nitrazine or fern test. • Maternal or fetal instability. • Actively seizing
??Questions?? 5. The patient with postpartum fever may have any of the usual types of infection, or may have fever related to the postpartum state. Causes of fever related to the postpartum state that should be considered include which of the following: • pelvic thrombophlebitis. • endometritis. • episiotomy infection. • surgical wound infection after cesarean section. • all of the above ANSWERS: DDDBE