Ventricular Assist Device Exit Site Care
260 likes | 693 Vues
Ventricular Assist Device Exit Site Care. Nicole Graney, MSN, CNS-BC VAD Coordinator Advocate Christ Medical Center. Ventricular Assist Device Percutaneous Lead. Referred to also as: Driveline Perc Lead

Ventricular Assist Device Exit Site Care
E N D
Presentation Transcript
Ventricular Assist DeviceExit Site Care Nicole Graney, MSN, CNS-BCVAD Coordinator Advocate Christ Medical Center
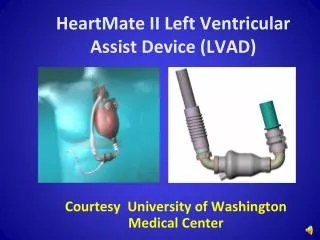
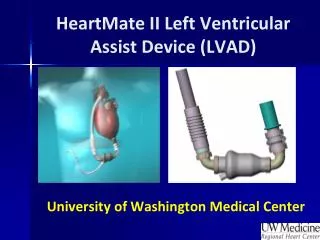
Ventricular Assist DevicePercutaneous Lead Referred to also as: Driveline Perc Lead This lead connects the implanted device to the external controller which provides power to the pump and controls operation. Thoratec Corporation. HeartMate II Patient Handbook, 2008.
Percutaneous Lead The outside of the lead is covered with a special material (velour) that allows skin cells grow into it. A well-healed exit site can lower the risk of infection.
Exit Site The exit site is the location where the percutaneous lead goes out through the skin
Caring for the Perc Lead Exit Site • Keep the exit site clean, dry and covered. • Ensure patient and caregiver performing proper hand washing and “aseptic technique” when changing bandage or handling the exit site. • Keep perc lead stabilized using Stabilization Belt. • Protect the system controller from falling or from pulling on the lead. • Don’t allow the perc lead to catch or snag on anything that will pull or move the lead. • Check lead daily for signs of damage. • Report any concerns of damage or infection to patient’s VAD Coordinator.
Assessment of Exit Site • Tissue in-growth • Drainage • Surrounding Tissue
Assessment of Exit Site • Most VAD infections began at the perc lead exit site. • Accurate assessments allow the health care provider to identify and promptly treat driveline infections. • If any concerns, please contact patient’s VAD coordinator.
Tissue In-growth • Refers to amount of tissue growing into the perc lead. • If complete in-growth, should not be able to retract back on abdomen and expose any velour • Can be describe in percentages • Anywhere from 0 to 100 % • Problem: Percentages may differ between person assessing • Can be described as Partial or Complete • Can specify where tissue in-growth is using hours on a clock using circumference of driveline as the clock. • Complete in-growth from 2-6 o’clock position
Tissue In-growth 100 % Tissue In-growth Or Complete Tissue In-growth
Drainage • Important to Note • Amount • Color • Odor • Consistency
Surrounding Tissue Appearance of surrounding tissue may indicate presence of early infection, even without drainage or fever. Note any erythema, edema, blisters, hypergranulation tissue etc.
Infection • Infection is one of the common causes of mortality in patient’s with VADs. • The treatment of VAD related infections negatively impacts patient’s quality of life and length of survival with VAD. • Prevention of infection is one of the primary goals of patient management.
Risk for Infections • Patients are at an increased risk for infection. • Chronic HF, poor nutrition, advanced age, other co-morbidities (DM, COPD etc.). • Presence of foreign body (VAD and perc lead), trauma to exit site, tension to wound edges, poor dressing care technique.
Signs of Symptoms of Infection • Localized Exit Site: • Redness, warmth, tenderness • With or without positive cultures • New or increased drainage • Severe Exit Site Infections or Pocket Infections: • Fever, Elevated White Blood Cell Count • Purulent drainage • Pain at exit site or over device • Positive wound cultures • Fluid surrounding perc lead up to the device • Patient may become septic as a result • Fluid over device, erythema over pocket
TreatmentLocalized • Increase frequency of driveline dressing changes if drainage present • Immobilize perc lead • Start antibiotics if culture positive • Monitor frequently as outpatient • Initiate aggressive wound care modalities: silver impregnated dressings, ultrasound mist therapy.
Treatment Severe Exit or Pocket Infections • Hospitalization • IV antibiotics • Aggressive Wound Care Modalities • Surgical Drainage of fluid collection
TreatmentDevice Infection/Sepsis • Surgical implantation of antibiotic beds • Expose device to allow for constant drainage • Device Exchange as last resort
Complications of Persistent Exit Site Infections • Sepsis • Exposure of device • Stroke • Death
Trauma • Trauma to perc lead either due to pulling, tearing, or dropping of equipment may lead to infection, damage of equipment, or pump stoppage.
Perc Lead Fracture • If complete severing of electrical leads, the pump will STOP! • Patients may not survive pump stoppage, or may go into cardiogenic shock