Ventricular Assist Devices
Ventricular Assist Devices. Overview, Patient Management and Emergency Care Timothy Ryan, APRN-NP. Learning Objectives. Identify the components, their function, & theory of device operation of the LVAD Describe the path blood follows in patients with the LVAD

Ventricular Assist Devices
E N D
Presentation Transcript
Ventricular Assist Devices Overview, Patient Management and Emergency Care Timothy Ryan, APRN-NP
Learning Objectives • Identify the components, their function, & theory of device operation of the LVAD • Describe the path blood follows in patients with the LVAD • List two potential complications associated with the LVAD • Identify the purpose and function of the System Controller • Discuss Nursing Care of a Patient with a LVAD • Describe appropriate interventions in the event of an emergency
Indication for Use • Bridge to Transplant • Non-reversible left heart failure • Imminent risk of death • Candidate for cardiac transplantation • Destination Therapy • Not candidate for transplant • Lifelong support
Considerations • Contraindication: • Inability to tolerate anticoagulation • Other considerations: • Nonreversible end organ failure • Acceptance of blood products • Pregnancy • Support system • Compliance history
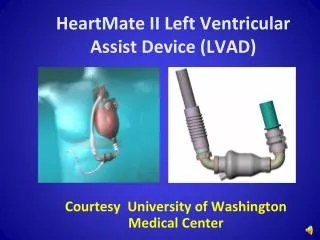
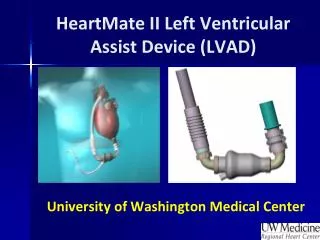
HeartMate II LVAS System Components • HM II Components: • Implantable titanium blood pump • System Controller • System Components: • System Monitor • Display Module • Power Sources • Power Module • Batteries & Clips • Accessories • Shower Bag • Travel Bag
HeartMate II LVAS • Valveless • Afterload sensitive • Follows native LV pulse • Pump flow varies over the cardiac cycle
Relatively Simple Design Valveless Only one moving part, the rotor Blood immersed bearings designed for minimization of blood damage All motor drive and control electronics are outside of the implanted blood pump Speed range: 6,000 to 15,000 rpm Flow range: 3 – 10 L/min HeartMate II LVASKey Design Features
Internal View Rev. 12.0 (3/24/04)
Blood Flow Path • Inflow from LV • Inlet Stator • 3 vanes “straighten” the flow before it enters the rotor • Rotor • Propel blood toward outflow & spins it radially imparting kinetic energy • Outlet stator • “Straightens” flow as leaves rotor and pressure is further increased • Outflow to ascending aorta
Pump Flow Principles • Pump flow is a function of: • The speed of the rotor ↑Speed → ↑Flow ↓Speed → ↓ Flow • The difference in pressure across the pump ↑ Pressure gradient → ↓ Flow ↓ Pressure gradient → ↑ Flow At any given speed, increased B/P will decrease flow
Speed mean (range) 9,400 rpm (8,000 – 13,000) Flow mean (range) 5.5 lpm (3.3 – 7.8) Typical Pump Parameters
Key Points • Valveless pump • Retrograde flow will occur if the pump stops • Degree of retrograde flow is determined by pressure differential across the pump • Similar to acute aortic regurgitation • Significant negative pressures can be produced when insufficient blood is provided to the pump • Dehydration or RV failure can cause suction events • Suction events can cause arrhythmias
Equipment Overview System Controller Power Sources System Monitor Display Module
Microprocessor that: Delivers power to the pump Controls pump speed and power Monitors, interprets & responds to system performance Performs diagnostic monitoring Indicates hazard and advisory alarms Provides complete backup system Event recording capability System Controller
System Controller Perc Lock • Design implemented to prevent accidental percutaneous lead disconnects from the system controller
HeartMate II Pocket System Controller • Safety by Design • Backup battery • Prioritized visual alarms with clear, actionable instructions • Driveline diagnostic capability • Programmed for use in 37 languages • Designed for an active lifestyle • Lightweight and compact with single-side cable design • Durable, shock-resistant outer case, cables, and electronics • Intuitive, discreet, and comfortable interface
HeartMate II System Controller • Delivers power to the pump • Controls and monitors system operation • Identifies alarm conditions and initiates Hazard and Advisory Alarms • User Interface displays the following available in 37 languages: • Pump parameters (Flow, Speed, Power, PI) and status of Backup Battery charge • Visual alarms with clear, actionable instructions • Accessible alarm history of last six non-transient alarms • Display Module no longer required • Backup battery housed within the controller • Driveline diagnostic capability • Records alarm data and device performance (240 events)
Power Module • Supplies mains power to LVAD • Serves as the electrical interface between the System Controller and the System Monitor or Display Module • Weights only 10 pounds • Can run off of car power • Provides 30 minutes of backup power • Takes 12 hours to recharge • Keep plugged into grounded outlet at all times • Internal battery must be changed yearly
Batteries • 14-volt Li-Ion Battery • 10+ hours of support on a pair of batteries • Four hours recharge for fully discharged battery • Service life of greater than 2 years (auto recalibration)
Parameters Pump Mode Pump Speed (rpm) PI (Pulsatility Index) Estimated Flow (lpm) Too low “---” Too high “+++” Power (watts) Alarm conditions Highest priority alarm message alternates with flow and power Display Module
Post Op Complications • Hypovolemia • Right Heart failure • Pulmonary hypertension • Cardiac tamponade • Bleeding • Arrhythmia • Infection • Hemolysis • Thromboembolism • Neurologic dysfunction
Potential Late Complications • Hypovolemia • Arrhythmia • Thromboembolism • Infection • Psycho-social issues • Neurological dysfunction
Patient Assessment • Patient assessment includes: • Pump function • Pump speed, flow, motor power, pulse index (PI) • Percutaneous lead connection to system controller and percutaneous lead lock in locked position • Exit site status, immobilization of percutaneous lead • Vital signs, peripheral circulation • Mental status, level of consciousness • Lab work
Exit Site Care • Dressing change • Every Monday and Thursday • Use Sterile Technique • Sterile Gloves and mask • Chlorohexadine Prep • Sterile dressing
Care of the Percutaneous Lead • Damage to the percutaneous lead, depending on the degree, may cause the pump to stop • Do not severely bend, kink or twist the percutaneous lead • Do not “catch” the percutaneous lead in the zipper of the carrying case • Allow for a gentle curve of the percutaneous lead. • Do not severely bend the lead multiple times or wrap it tightly. • Keep the percutaneous lead clean • Wipe off any dirt or grime • If necessary, use a towel with soap and warm water to gently clean the percutaneous lead • Never submerge the lead or other system components in water or liquid
Care of the Percutaneous Lead • Do not pull on or move the lead at the exit site • Be mindful of where the system controller is at all times • Protect the controller from falling or pulling on the lead • Don’t allow the percutaneous lead to catch or snag on anything that will pull on or move the lead • Check the percutaneous lead daily for signs of damage • Cuts, holes, tears
Warnings & Restrictions • No excessive jumping or contact sports • No swimming • No exposure to MRI • Avoid strong static discharge (i.e. TV, computer screens, vacuuming carpets) • No pregnancy
Patient Assessment • Vital Signs • No pulse • No blood pressure • Cannot use automatic blood pressure machine • Doppler used to get mean arterial pressure • Target mean pressure of 70-90 mmHg • Arterial line waveform dampened
Patient Care Arrhythmias • Affect pump function • Can be caused by mechanical irritation of ventricular wall by inflow catheter • Must be treated using usual care • ICD’s are turned back on after implant • Cardioversion or defibrillation WILL NOT affect VAD function
Patient Care Anticoagulation • Because of risk of clot formation in pump • Warfarin with target INR 2.0 to 3.0 (higher if other conditions) • Also on aspirin and dipyridamole therapy
Emergency Care • Acute Pump Failure • Depleted Batteries • Loss of home power and not switched to battery • Controller Failure • Redundant System • Driveline Failure • Pump Failure
Emergency Care • Acute Pump Failure • Causes acute regurgitation to LV • If some LV function, will maintain some blood pressure, but will most likely be in shock • If minimal LV function, regurgitate flow will cause LV to dilate leading to VF • Need to restart pump as soon as possible • 10 minute rule
Emergency Care Cardiopulmonary Resuscitation • May perform cardioversion or defibrillation as needed. Will not affect VAD or controller • No CPR • Unless last resort • May dislodge inflow or outflow cannulas resulting in hemorrhage • Treat like cardiogenic shock if pump failure
Emergency Care Routing of Patients • Most patients will need to be transferred to The Nebraska Medical Center. • May first present to local ED for stabilization then transferred to The Nebraska Medical Center, if needed. • Other centers will not be able to treat pump related issues • Toll-Free Emergency Contact: 855-823-8662
Exercising And Cardiac Rehabilitation • Need to have doppler to evaluate blood pressure • No limitations to equipment used • Limit exercise to no higher than Borg level of 13 • Initially may have higher means • Will decrease over time • Strongly encourage Phase III
The Nebraska Medical Center MCS Program Top 15% of Implanting Centers in the United States
Success Stories • http://www.omaha.com/article/20111025/NEWS2001/710199974 • http://www.youtube.com/watch?v=-zALZGINfAU • http://youtu.be/539A2dMOGK8