Download
1 / 20
230 likes | 631 Vues
Iron Deficiency Anemia. General Medicine Conference August 11, 2008. Epidemiology. The most common nutritional deficiency worldwide Prevalence up to 70% in developing countries Under 20% in North America and Europe

E N D
Iron Deficiency Anemia General Medicine Conference August 11, 2008
Epidemiology • The most common nutritional deficiency worldwide • Prevalence up to 70% in developing countries • Under 20% in North America and Europe • Greatest prevalence in US is in toddlers 1-2 yrs old and girls/women from 12-49 yrs.
IDA • Don’t overlook anemia. • Most often associated with blood loss (obvious or occult). • “In a study of 9024 participants in the NHANES I study, men and postmenopausal women with iron deficiency anemia had an increased risk of being diagnosed with a gastrointestinal malignancy within the subsequent two years (relative risk versus non-iron deficient controls 31, 95% CI 9-107)”
IDA • “In a report dealing with 148 consecutive patients with iron deficiency anemia, 18 patients (12 percent) were found to have a malignant tumor. Using multivariate analysis, the odds ratio for the presence of malignancy in a patient with a serum ferritin ≤10 microg/L and an LDH >250 U/L, when compared with patients having a ferritin >10 and an LDH <250, was 74 (95% CI 7-776)”
Iron Metabolism • Humans are unable to excrete excess iron, so iron balance is regulated by the control of iron absorption. • Based on the level of body iron stores and the extent of erythropoiesis.
Molecular Iron Metabolism • Transferrin is the physiologic carrier of iron through the plasma and extracellular fluid. • Single chain glycoprotein with two lobes. • Apotransferrin = empty lobes • Monoferric transferrin, biferric transferrin… • Transferrin saturation = percentage of the available iron-binding sites on transferrin that are occupied by iron atoms.
Molecular Iron Metabolism • Ferritin is a protein in the cytoplasm of nearly all cells…“a spherical shell that can store as many as 4,500 atoms of iron.” • Most ferritin is found in macrophages, hepatocytes and developing RBCs. • Best for diagnosis of iron deficiency. • Gold standard is bone marrow biopsy.
Molecular Iron Metabolism • Serum iron (SI) is usually low in ID, transferrin (TIBC) then is usually high… • SI/TIBC = transferrin saturation (usually low) • Second to ferritin in diagnosing iron deficiency. SI is not specific and transferrin varies with clinical states and meds.
Increased iron requirements GI blood loss Menstrual bleeding Respiratory tract Avid blood donation Growth during childhood and pregnancy/lactation Inadequate iron supply Diet Impaired absorption Women may have diets that contain little iron and take calcium, an inhibitor of iron absorption. Etiology of IDA
History Age and gender Diet (vegetarian) Blood donations Heavy menses Paradoxic weight loss Chronic blood loss Pica (pagophagia) IBD symptoms Dysphagia Sore tongue Restless leg syndrome Physical exam Weakness, dizziness, fatigue, pallor, other nonspecific complaints General to all anemias Blue sclerae Esophageal web Koilonychia Specific to IDA Diagnosis
Diagnosis (Laboratory) • All about serum ferritin • “There is no clinical situation other than iron deficiency in which extremely low values of serum ferritin are seen.” • The traditional cutoff for ferritin has been 15 ng/ml. (sens = 59%, spec = 99%) • Increasing the cutoff up to 41ng/ml changes the sensitivity and specificity to 98%
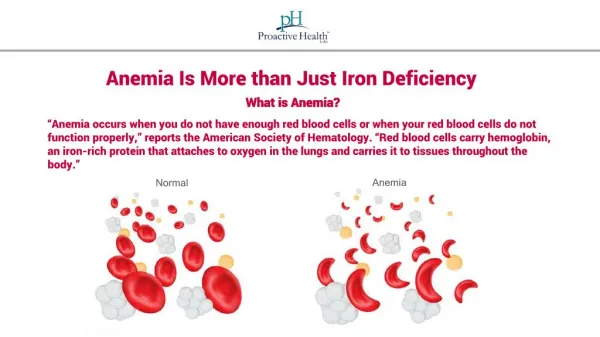
Diagnosis (Labs) • “IDA is the only microcytic hypochromic anemia associated with lack of iron stores.” • Usually must differentiate IDA from AoCD • In the presence of inflammation the serum ferritin can also be used to reliably detect iron sufficiency (at levels greater than 100ng/ml)
Diagnosis (Labs) • Ferritin is usually elevated roughly 3 times by inflammatory conditions. • Patient with active RA and ferritin of 60 ng/ml may be considered iron deficient. • Problem may arise if there is a patient with a chronic inflammatory state who has microcytic anemia with a ferritin value between roughly 60 to 100ng/ml. • SI and TIBC should be low in AoCD but this is not always reliable.
Diagnosis (Labs) • The serum transferrin receptor concentration is possibly a way to differentiate the two as it offers a quantitative measurement of erythropoietic activity.
Treatment • Ferrous sulfate, 325 mg po 2 or 3 times per day. • Duration of 6 months (anemia may correct in 1 or 2 months but full therapy needed to replete stores) • On empty stomach if tolerated.
Treatment • Consider IV iron replacement in those IDA patients refractory to oral therapy. • Absorption problems • Small bowel resection • ESRD on HD • Nonadherence • Ongoing blood loss that cannot be stopped (Cancer) • Iron sucrose 125 mg/d iv infusions • Dose (mg) = (15 - patient's hemoglobin in g/dL) × (body weight in kg) × 3
Treatment • Do not give IDA patients erythropoietin until documenting that iron stores are adequate (ferritin levels).