
Asthma
Asthma. The University of Kansas Medical Center Family Care Clinic Danielle Herrmann. Epidemiology and Etiology. Most prevalent chronic disease of childhood Very prevalent in 5-17 year olds Puerto Ricans and non-hispanic blacks have an increased risk

Asthma
E N D
Presentation Transcript
Asthma The University of Kansas Medical Center Family Care Clinic Danielle Herrmann
Epidemiology and Etiology • Most prevalent chronic disease of childhood • Very prevalent in 5-17 year olds • Puerto Ricans and non-hispanic blacks have an increased risk • 10.1 million workdays and 12.8 school days missed • 1.77 million emergency room visits • Economic burden of $19.7 billion • Inherited component • Environmental factors
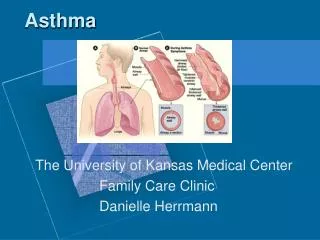
Pathophysiology • Inhaled antigens induce a type 2 T-helper CD4 response • Antigens taken up by APC --> activation of the TH2 response • Leading to B cell production of IgE and proinflamatory cytokines and chemokines that recruit and activate eosinophils, neutrophils, and alveolar macrophages • Subsequent exposure to the antigen results in cross linking of cell-bound IgE in mast cells and basophils • This causes the release of histamine, leukotrienes and prostaglandins
Clinical Presentation and Diagnosis- Chronic Asthma • Symptoms- • Dyspnea, cough • Wheezing and chest tightness (episodic, seasonal, or with known triggers) • Symptoms may occur more at night, early in the morning, or with exercise • Many patients with intermittent asthma symptom free and normal pulmonary function between exacerbations • Laboratory tests- • Increased IgE and eisinophils- but not diagnostic • Signs- • End-expiratory wheezing and dry cough
Clinical Presentation and Diagnosis- Acute Asthma • Symptoms- • Dyspnea, cough, shortness of breath, chest tightness • Anxious • Mental status changes • Laboratory tests- • Arterial blood gases • CBC with differential in patients with fever or purulent sputum • Serum electrolytes • Signs- • Tachypnea • Tachycardia • Bradycardia • Wheezing with expiration and inspiration • Hyperinflation, and use of accessory muscles to breathe, cyanosis, and diaphoresis
Factors Affecting Asthma Severity • Allergens • Environmental chemical exposure • Environmental Pollution • Tobacco Smoke exposure • Contaminant rhinitis • GERD • Non-selective B-Blockers should be avoided in asthmatics
Intermittent • Symptoms • ≤2 days/week • Nighttime Awakenings • ≤2x/month • Short-acting beta 2 agonist use for symptom control • ≤2 days/week • Interference with normal activities • None • Lung Function • Normal FEV1 between exacerbations • FEV1> 80% predicted • FEV/FVC normal • Exacerbations requiring oral systemic corticosteroids • ≥2/year
Mild Persistent • Symptoms • >2 days/week but not daily • Nighttime Awakenings • 3-4x/month • Short-acting beta 2 agonist use for symptom control • >2 days/week but not daily, and not more than 1x per day • Interference with normal activities • Minor limitation • Lung Function • FEV1> 80% predicted • FEV/FVC normal • Exacerbations requiring oral systemic corticosteroids • >2/year
Moderate Persistent • Symptoms • Daily • Nighttime Awakenings • >1x/week but not nightly • Short-acting beta 2 agonist use for symptom control • Daily • Interference with normal activities • Some limitation • Lung Function • FEV1> 60% but <80% predicted • FEV/FVC reduced 5% • Exacerbations requiring oral systemic corticosteroids • >2/year
Severe Persistent • Symptoms • Throughout the day • Nighttime Awakenings • Often 7x/week • Short-acting beta 2 agonist use for symptom control • Several times per day • Interference with normal activities • Extremely limited • Lung Function • FEV1> 60% • FEV/FVC reduced 5% • Exacerbations requiring oral systemic corticosteroids • >2/year
Step Wise Approach for managing Asthma in youths >12 years of age and adults • Use of SABA >2 days a week for symptom relief (not prevention of EIB) generally indicates inadequate control and the need to step up treatment • Step down possible if symptoms controlled for 3 months
Step 1 Used in patients with Intermittent Asthma • Preferred • SABA PRN
Step 2 • Used in patients with Mild Persistent Asthma • Preferred • Low Dose ICS • Alternative • Cromolyn • LTRA • Nedocromill • Theophylline
Step 3 Used in patients with Moderate Persistent Asthma • Preferred • Low-dose ICS+LABA • Medium-dose ICS • Alternative • Low-dose ICS + either LTRA, Theophylline, or Zileuton
Step 4 • Used in patients with Severe Persistent Asthma • Preferred • Medium-dose ICS + LABA • Alternative • Medium-dose ICS + either LTRA, Theophylline, or Zileuton
Step 5 • Used in patients with Severe Persistent Asthma • Preferred • High-dose ICS + LABA • Alternative • Consider Omalizumab for patients who have allergies
Step 6 • Used in patients with Severe Persistent Asthma • Preferred • High-dose ICS + LABA+ oral corticosteroid • Alternative • Consider Omalizumab for patients who have allergies
Special Populations • Pregnancy: • 8% of pregnant women are affected by asthma • Risk to baby • Budesonide is the preferred ICS • Albuterol is the drug of choice
Special Populations Cont… • Aspirin Sensitive • Exercise induced asthma • Patients encouraged to warm up • Gradually decreasing and increasing intensity • Pretreatment with albuterol • Pretreatment with leukotriene
Asthma Exacerbations -Assess Severity -Initial treatment -Good response, Incomplete Response, Poor Response
Nonpharmacologic Therapy • Goals for asthma treatment shared • Patient education • At time of diagnosis and tailored to meet individual patient needs
Pharmacological therapy: B2 Adrenergic Agonists • Relax airway smooth muscle • Increase mucociliary clearance • Stabilize mast cell membranes • Adverse effects: • Tachycardia • Tremor • Hypokalemia
Pharmacological therapy: Short-Acting Inhaled B2 Agonists • Most effective agent for reversing acute airway obstruction • Drug of choice for treating acute severe asthma and chronic asthma • Onset of <5 minutes • Duration 4-6 hours
Pharmacological therapy: Short-Acting Inhaled B2 Agonists -Albuterol HFA 90mcg/puff (Proair HFA, Ventolin,Proventil) - 0-4years: 1-2 puffs 5 minutes before exercise and 2 puffs every 4-6 hours PRN - 5- adult: 2 puffs 5 minutes before exercise and 2 puffs every 4-6 hours PRN • Albuterol nebulizer solution: • 0-4 years: 0.63-2.5mg in 3 mL saline every 4-6 hours • 5-adult: 1.25-5mg in 3mL saline every 4-8 hours as needed
Pharmacological therapy: Short-Acting Inhaled B2 Agonists • Levalbuterol HFA 45mcg/puff (Xopenex) • 0-4 years: N/A • 5- adult: 2 puffs 5 minutes before exercise and 2 puffs every 4-6 hours PRN • Levalbuterol nebulizer solution: • 0-4 years: 0.31-1.25mg in 3 mL saline every 4-6 hours • 5-11years: 0.31-0.63mg every 8 hours as needed • Adult - 0.63-1.25mg every 8 hours
Pharmacological therapy: Long-Acting Inhaled B2-Agonists • Provide up to 12 hours of bronchodialation • Approved for chronic prevention • Onset of 30 minutes • Add on therapy only • Many of these products also available in combination products
Pharmacological therapy: Long-Acting Inhaled B2-Agonists • Salmeterol DPI 50mcg/blister (Serevent): • Not indicated in children under 4 • 5-adult- Contents of one blister every 12 hours • Formeterol PI 12 mcg/capsule: • Not indicated in children under 4 • 5-adult- Contents of one blister every 12 hours
Combined medication • Fluticasone/Salmeterol DPI (Advair diskus and HFA) 100mcg/50mcg, 250mcg/50mcg, 500mcg/50mcg HFA MDI 45mcg/21mcg, 115mcg/21mcg, 230mcg/21mcg • 1 inhalation twice a day • Budesonide/Formoterol HFA MDI (Symbicort) 80mcg/4.5mcg, 160mcg/4.5mcg • 2 puffs twice a day
Pharmacological therapy: Inhaled Corticosteroids • Preferred therapy for all forms of persistent asthma in all ages • Targeted drug delivery to the lungs • Clinical effects apparent after 2 weeks • Local effects: oral candidiasis, cough, hoarse voice, dysphonia, adrenal suppression, decreased bone mineral density, skin thinning, cataracts, easy bruising
Pharmacological therapy: Systemic Corticosteroids • Effective as long term treatment and rescue medication • Serious potential side effects include • Cornerstone of treatment for worsening asthma and patients not responding
Pharmacological therapy: Systemic Corticosteroids • Methyprednisolone- 2,4,6,8,16,32 mg oral tablets • Prednisolone (- 5mg oral tablets; 5mg/mL and 15mg/5mL oral liquids • Prednisone- 1, 2.5, 5, 10, 20, 50mg tablets; 5mg/mL and 5mg/5mL oral liquid • 0-4years- short course burst “1-2mg/kg/day PO, max 60mg/day po for 3-10 days • 5-adult- Short course burst 40-60mg/day po as a single or divided dose for 3-10 days
Pharmacological therapy: Anticholinergics • Inhibit the effects of acetylcholine on muscarinic receptors in the airways • Bothersome side effect profile: blurred vision, dry mouth, urinary retention, and constipation • Not absorbed systemically
Pharmacological therapy: Anticholinergics • Ipratropium HFA (Atrovent)- • Only for use in adults • 2-3 puffs every 6 hours, nebulizer- 0.25mg every 6 hours • Ipratropium with albuterol • Only for use in adults • 2-3 puffs every 6 hours, nebulizer- 3mL every 6 hours • Tiotropium HFA (Spiriva)- -- Onset of action of 30 minutes • Little evidence in asthma
Pharmacological therapy: Leukotriene Modifiers • Inhibit 5-lipoxygenase or competitively antagonize effect of leukotriene D • Improve FEV and decrease symptoms • Less effective than ICS
Pharmacological therapy: Leukotriene Modifiers • Montelukast 4 or 5mg chewable tabs or granule packs, and 10mg tabs (Singular) • 0-4 years old- 4mg tablet at bedtime • 6-14 years old- 5mg tablet at bedtime • Adult 10mg tablet at bedtime
Pharmacological therapy: Leukotriene Modifiers • Zafirlukast 10 or 20mg tablets (Accolate) • Take with meals • 5-11 year olds- 10mg BID • Adult dose- 40mg daily
Pharmacological therapy: Leukotriene Modifiers • Zileuton 600 mg tablets (Zyflo) • Only for use in adults 4 times a day • Monitor hepatic enzymes
Pharmacological therapy: Cromolyn and Nedocromil • Inhaled inflammatory agents • Inhibit release of mediators from mast cells • Alternatives to ICS treatment • Maximal benefit after 4-6 weeks • Adverse effects= cough, wheezing, bad taste, and headache
Pharmacological therapy: Cromolyn and Nedocromil • Nedocromil (Tilade, Alocril) • 2 puffs 4 times a day • Once controlled frequency of dosing can be reduced • Cromolyn • 2 puffs 4 times a day • Or one ampule 4 times a day
Pharmacological therapy: Methylxanthines • Causes bronchodilator by inhibiting phosphodiesterase and antagonizing adenosine • Limited use • Increase risk for adverse drug reactions with serum levels of > 15mg/L • Large number of drug interactions
Pharmacological therapy: Methylxanthines • Theophylline • 10mg/kg/day with a max dose of 16mg/kg/day (same for 0-adult) • Monitor for serum theophylline level
Pharmacological therapy: Omalizumab (Zolair) • Recombinant humanized monoclonal anti-IgE antibody • Inhibits binding of IgE to receptors on mast cells and basophils • Positive skin test or invitro reactivity to perennial allergens • Decreases ICS use • High cost • Side effects: bruising, pain, stinging, itching, burning, and anaphylactic reactions
Pharmacological therapy: Omalizumab • Omalizumab subcutaneous injection • Adults 150-375mcg SC every 2-4 weeks depending on body weight and pretreatment serum IgE levels • Monitor for anaphylaxis • Do not administer more than 150mcg per injection site
Patient Monitoring • 1.Monitoring of asthma control • 2.Establishing goals of therapy • 3.Periodic assessment and monitoring of asthma control, including • Signs and symptom • Pulmonary function, via spirometry or peak flow monitoring • Quality of life • History of exacerbations • Pharmacotherapy (adherence and side effects) • Patient-provider communication and patient satisfaction
Inhaler Technique • Remove the cap • Shake the inhaler • Tilt your head back slightly and breathe out slowly • Position the inhaler 1-2 inches away from mouth, in a chamber, or in the mouth • Press down on the inhaler to release medication while starting to breathe in slowly • Breathe in for 3-5 seconds (slowly) • Hold breath for 10 seconds to allow medication to reach all the way deep into lungs • Repeat puff. Wait one minute between puffs will allow the second one to penetrate your lungs better • Spacers and chambers are very useful and are recommended for young children and older adults and for use with corticosteroids
Common inhaler mistakes to watch for • Breathing out while pressing inhaler • Inhaling quickly • Breathing in trough nose • Pressing down before starting to inhale • Stopping inhalation as pressing down on inhaler • Pressing inhaler more than once during inhalation • Not breathing evenly and deeply





















