Comprehensive Guide to Immunisation: Types, Methods, and Effectiveness
Learn about passive and active immunisation, types of vaccines, UK's immunisation schedule, and novel vaccination approaches. Understand how vaccines work, their limitations, advantages, and disadvantages.

Comprehensive Guide to Immunisation: Types, Methods, and Effectiveness
E N D
Presentation Transcript
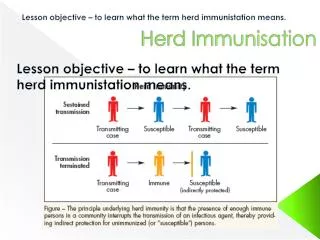
Immunisation The induction of protection or “immunity” to infection
• Traditionally 3 types of vaccines used-whole killed, toxoids, live attenuated. • Novel methods of vaccine production •UK Immunisation schedule (current) •Do vaccines work?
Immunisation •Passive Immunisation •Active Immunisation or Vaccination
Passive Immunisation The administration of pre-formed “immunity” from one person or animal, to another person Limitation- Antibody mediated Advantages- Gives immediate protection Effective in immunocompromised patients Disadvantages Short-lived Possible transfer of pathogens “Serum sickness” on transfer of animal sera
Passive Immunisation Specific Immunoglobulin: • Human tetanus immunoglobulin (HTIG) Rapid protection of exposed individuals • Human rabies specific Ig Used after exposure to rabies to give protection until vaccine becomes effective •Human Hepatitis B Ig (HBIG) • Varicella Zoster Ig (VZIG)
Passive Immunisation Normal Immunoglobulin (HNIG) Prepared from pools of at least 1000 donors, contains antibody against measles, mumps, varicella, hepatitis A etc.
Active Immunisation(Vaccination) Traditionally, vaccines have been divided into: •Non-living vaccines (whole killed and toxoids) •Live attenuated Vaccines
Non-living Vaccines Whole Killed vaccines Bacteria or viruses grown in vitro and inactivated using an agent such as formaldehyde or b-propionolactone Non living vaccine does not cause infection, but the antigens contained in it induce an immune response which protects against infection. Toxoids Non-living vaccines can also be cell-free toxoids-inactivated toxins
Whole killed Vaccines Problems and limitations: •The organisms must be grown to high titre in vitro •Whole pathogens often cause excessive reactogencity •Immune responses are not always close to the normal response to infection, e.g no mucosal immunity, no CTL responses • Usually need at least 2 shots.
Non-living Vaccines Examples: Bacterial •Diphtheria-cell free formaldehyde treated toxin- rendered non toxic “toxoid” •Tetanus, toxoid, as above •Pertussis- killed whole bacteria, given with the two above as DTP. 3-doses. UK has now moved to acellular pertussis (aP) •Cholera- heat killed bacteria
Whole killed Vaccines Examples: Viral •Polio vaccine (Salk)-inactivated virus-IPV •Influenza vaccine-inactivated virus •Hepatitis A vaccine-inactivated virus •Rabies vaccine-inactivated virus
Live Attenuated Vaccines The organisms replicate within the host, and induce an immune response which is protective against the wild-type organism
Live Attenuated Vaccines Advantages: •Lower doses are required, so the scale of in vitro growth needed is lower •Immune response more closely mimics that following real infection •Route of administration may be more favourable •Fewer doses may be required
Live Attenuated Vaccines Problems and Limitations: •Often impossible to balance attenuation and Immunogenicity •Reversion to virulence? •Transmissibility? •Live vaccines may not be so attenuated in immunocompromised hosts
Live Attenuated Vaccines Examples: Bacterial Only 2. • BCG- Bacille Calmette Guerin. Mycobacterium bovis grown over many passages in vitro. Gives some protection against TB •Salmonella typhi- temperature sensitive strain given orally.
Live Attenuated Vaccines Examples: Viral • Poliomyelitis (Sabin)-widely used to bring polio to the brink of eradication • Vaccinia virus- used in billions of doses to eradicate smallpox due to cross-reactivity between itself and the variola virus. •Measles, Mumps and Rubella- 3 given together. • Rotarix, Rotavirus vaccine, introduced to UK July 1st 2013.
Pathogens lacking Vaccines Too numerous to list, but a few: HIV, malaria, Schistosomiasis, Leishmania spp, Herpes simplex Virus, CMV, RSV, Rhinoviruses, Group B streptococci, Meningococcus group B, M.leprae,
Pathogens lacking Vaccines Why so many? Various reasons- pathogen too hard to grow, killed pathogen not protective, impossible to obtain attenuated and suitably immunogenic strain, too many strains causing disease etc.
Novel approaches • Recombinant proteins • Synthetic peptides • Live attenuated vectors • DNA vaccines • Polysaccharide-protein conjugates.
Recombinant proteins Produced from bacteria, yeast, insect or mammalian cells •Avoid the problem of having to grow pathogen in vitro •Major difficulties are finding a protein or proteins which are protective, and generating a strong enough immune response. • Two examples on the market, Hepatitis B surface antigen, and HPV vaccines Cervarix and Gardasil.
Hepatitis B Virus Dr L Stannard Science Photo library
Synthetic peptides • Avoid the need for pathogen growth • Identifying protective epitopes is a problem • Inducing a strong response can be a problem • Inducing a broad response can be a problem • No examples on the market
Live attenuated vectors Express protein from the pathogen in a vector which is known to be attenuated and safe, e.g • Vaccinia • BCG • Adenovirus None on the market Potential problems in immunodeficient people
Vaccinia virus •Progressive vaccinia Occurred in about 1.6 people per million vaccinated during the smallpox eradication campaign. These were likely immunocompromised people
Live attenuated vectors Attenuated, genetically stable vaccine Vector able to take additional Foreign DNA Insert DNA encoding protective Antigen of pathogen, e.g HIV
DNA Vaccines Express protein from the pathogen in a mammalian expression plasmid which is then injected, so that protein is expressed. • Avoid the need to grow the pathogen • No live organism involved • DNA is cheap to produce • Problem is poor immunogenicity • None on the market
Heterologous Prime-Boost • Prime the response with a DNA vaccine • Boost with a vectored vaccine or recombinant protein • Works well experimentally and in trials
S.pneumoniae Dr Immo Rantala Science Photo library
T independent antigens • Bacterial capsular polysaccharides cannot be processed + presented on MHC class II • No T cell help • Antibody response of low magnitude • Low affinity • Predominantly IgM • Little or no boosting on secondary exposure • Infants respond especially poorly and are major target group for these vaccines • e.g. Haemophilus influenzae • Neisseria meningitidis • Streptococcus pneumoniae
Hib polysacc Diphtheria toxoid Hib ps specific B cell B cell B cell T cell TCR HELP Conjugation of TI antigens to proteins • Hib polysacc specific B cells bind polysaccharide and internalise whole conjugate, including protein • Polysaccharide cannot be processed, but protein is and peptides derived from it are expressed on cell-surface with MHC class II • Polysaccharide specific B cell receives help from DT specific T cell • Strong antibody response even in infants, including IgG Proliferation Isotype switching etc.
Conjugate Vaccines •Neisseria meningitidis type C- polysaccharide-protein conjugate vaccine •Streptococcus pneumoniae-23-valent polysaccharide vaccine or 7-valent conjugate •Haemophilus influenzae type B (HiB)- Polysaccharide protein conjugate vaccine
When designing a vaccine, youneed to understand the disease pathogenesis Malaria- A major killer of increasing importance due to drug and insecticide resistance
Malaria Targets for vaccination • Sporozoite stage • A few minutes from entry of the parasites into the bloodstream to invasion of the liver cells. A vaccine based solely on the sporozoite stage needs to be 100% effective, is aimed at preventing infection. Because of the time available protection will probably depend upon maintaining high levels of antibody.
Malaria Targets for vaccination • Erythrocytic stages • A vaccine based solely on the erythrocytic stages would not prevent infection. Since it is erythrocytic stages that cause disease, decrease in total parasitaemias (1% of red cells infected) should prevent disease and death.
Malaria Targets for vaccination • Gametes • Gametes are taken into the mosquito and carry on with the insect part of the life cycle. Vaccination against gametes or gametocytes would give a transmission blocking vaccine. This is an altruistic vaccine.
Malaria Targets for vaccination • Toxins • Vaccines based on the toxins released by the erythrocytic stages might prevent disease without affecting parasitaemias. May allow development of immunity naturally without deaths.
Recent changes to the programme • July 1st 2013 Rotavirus vaccine for babies under 4 months • Live attenuated nasal flu vaccine for 2 year olds- roll out 2014. • Shingles vaccine for 70 year olds. September 2013. Live attenuated Varicella Zoster Virus Vaccine • Teenage boost of Men C vaccine (14 years)
Upcoming changes? Group B meningococcus vaccine “Bexsero” under consideration. Recombinant protein vaccine.
Older people • PPV, Pneumococcal Polysaccharide vaccine offered from age 65. • Seasonal influenza vaccine offered annually • Shingles vaccine offered age 70