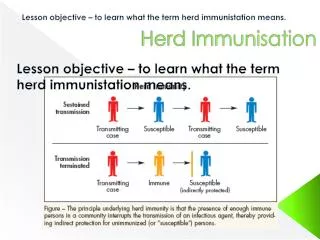
Vaccines and Immunisation
Vaccines and Immunisation. Medical Microbiology SBM 2044. Immunisation. Decrease in the incidence of infectious diseases since the middle 19 th century due to: improved sanitation the development of vaccines

Vaccines and Immunisation
E N D
Presentation Transcript
Vaccines and Immunisation Medical Microbiology SBM 2044
Immunisation • Decrease in the incidence of infectious diseases since the middle 19th century due to: • improved sanitation • the development of vaccines • Efficient water supplies and sewage disposal have reduces the transmission of typhoid, cholera, tuberculosis, typhus and plague agents. • Administration of vaccines have successfully eradicate smallpox; live, attenuated vaccines decrease the incidence of polio, measles, rubella, mumps and varicella. • Toxoid vaccines have caused a decline in diphtheria, tetanus and pertussis
Figure 1. Reported diphtheria cases in the Soviet Union and the Newly Independent States, 1920–1996.
INACTIVATED VACCINE ORAL VACCINE Figure 2. The incidence of paralytic poliomyelitis peaked in the US in 1952 with more than 20,000 cases. Because of the introduction of the killed IPV, or Salk vaccine, in 1954 and the live attenuated OPV, or Sabin vaccine, in 1961, the incidence has decreased to less than 10 cases per year in the US.
Is there any drawbacks of vaccinations? • Infectious diseases rising, despite the advances in sanitation and the use of vaccines. • Why? • Vaccines have not been developed for many pathogens, many which are major concerns of health e.g. HIV, respiratory diseases • Institutional public health control measures are difficult • Public concerns of the effectiveness and safety of vaccines
Terminology: • Vaccine : an immunizing agent derived from microorganisms, and can be either in the form of live, attenuated microorganisms, killed microorganisms and extracts of microorganisms • Attenuate : to reduce the severity, virulence or vitality • Toxoid :
Terminology: • Vaccine : an immunizing agent derived from microorganisms, and can be either in the form of live, attenuated microorganisms, killed microorganisms and extracts of microorganisms • Attenuate : to reduce the severity, virulence or vitality • Toxoid : an inactivated bacterial toxin that has lost its toxic properties but capable of inducing protective antibody
Approaches to Immunisation • Vaccinations to prevent infectious diseases have been greatly successful • The benefits include partial or complete protection against infections both for the vaccinated individuals, and for society as a whole • Benefits to society include the establishment and preservation of herd immunity, prevention of outbreaks and decrease in health care-related costs
Is vaccine safe? • No vaccine is completely safe or effective. • Immunisation practices must weigh the scientific evidence of the benefits for each person and for society against the potential costs and risks of the vaccination program
Strategies for immunisation • The choice of treating infectious diseases depends on: • The type of microorganisms • The age of the host • The time frame of contact between the host and the pathogen • Active immunisation – administration a microorganism, or a modified product of that microorganism to evoke an immunologic response; useful for preexposure control • Passive immunisation – administration of exogenously produced or preformed antibodies for the amelioration or prevention of infectious diseases; useful for postexposure control
Vaccines • Major types of vaccines:
Live vs. Killed vaccines • Vaccines are designed to stimulate antibody or cell-mediated immune responses directed against critical virulence factors of the organism • e.g. capsular polysaccharides of pneumococci, surface glycoprotein of hepatitis B virus and the haemagglutinin and neurominidase proteins of influenza virus • Immunity generated by a killed vaccine is not as effective nor long lasting as immunity stimulated by a live, attenuated vaccine
Live, attenuated vaccine • Cold-adapted influenza vaccine containing a weakened form of live influenza virus, and is administered by nasal spray (c.f. injection). Cold-adapted indicates that the virus can grow in the nose and throat but not in the lower resp t. where the temp is higher. • There is a risk that attenuated vaccine strain could revert to a more virulent strain in a susceptible host. E.g. vaccine-acquired paralytic poliomyelitis (VAPP) after millions of live polio vaccine was administered. • Live, attenuated rotavirus vaccine was found to be associated with an increased rate of intussuspection.
Age of Immunisation • Which serum antibody does the newborns directly received from their mothers? • Which secretory antibody is available in breast milk? • Humoral immunity responds well to protein antigens like DPT when given at 2 months of age, but not to certain polysaccharide antigens • Hepatitis B vaccine is immunogenic when given at birth • Live, attenuated viruses like MMR, are given after the 1st year of life because of the potential interference of maternally derived antibodies • The elderly > 65 years of age, have reduced capability to mount a primary antibody response to some antigens such as influenza virus and pneumococcus vaccine but able to mount secondary responses.
Malaysian Immunisation Recommended Immunisation Schedule for Infants and Children Not Immunised at the Recommended Time