Download
1 / 54
540 likes | 879 Vues
Neuromuscular disorders in children; making sense of the muscle, lung and brain. Sleep Course-Bristol Anirban Majumdar Consultant Paediatric Neurologist. Neuromuscular conditions. Overview Diagnosis Pathophysiology Surveillance and Treatments for NMD Trends and Survival in NM disorders

E N D
Neuromuscular disorders in children; making sense of the muscle, lung and brain Sleep Course-Bristol Anirban Majumdar Consultant Paediatric Neurologist
Neuromuscular conditions • Overview • Diagnosis • Pathophysiology • Surveillance and Treatments for NMD • Trends and Survival in NM disorders • Who goes into respiratory failure ? • The future • What we can do now • What we will try to do in the future • Clinical vignettes • Neuromuscular / respiratory- the interface
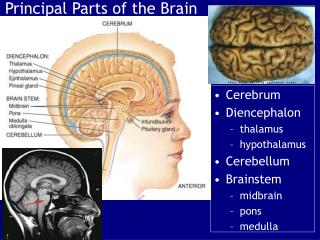
Brain Brain stem Spinal cord Anterior horn cell Nerve Neuromuscular junction Muscle
Multisystem disorders Ataxias Metabolic/ Mitochondrial Chanelopathies/ storage disorders SMA Demylinating/ Axonal Neuropathy Myesthenias Dystrophy Myopathy
Tone Hypotonia is a common diagnostic problem Hypotonia = floppiness
Weakness MRC evaluation of muscle power 0 – no contraction 1- flicker 2- Active movement with gravity eliminated 3- Active movement against gravity 4 - Active movement against gravity and resistance 5- Normal power + and – denotes through what range of normal movement
Recognizable patterns • Hypotonia + weakness = neuromuscular disease • Hypotonia without weakness may be • CNS • birth asphyxia • CNS malformations • Metabolic • lipidoses/MPS • amino-organic acidurias • peroxisomal • Connective tissue • Ehlers-Danlos/Marfan • OI • Chromosomal • PWS • Downs
Neuromuscular disorders • Presents with • floppiness • weakness • delayed motor milestones, • abnormal gait, clumsiness, • speech and swallowing difficulties • Respiratory, cardiac failure • Age : from newborn to adult life • Very wide range of severity and disability • Intelligence : very wide range
History Clinical examination Genetic analysis Biochemistry Immunology Muscle imaging EMG/NCV Muscle Biopsy Nerve biopsy Immunohistochemistry
Historical Notes 1851: Edward Merynon describes 10 cases in England 1861: Duchenne de Boulogne fils. De la paralysie atrophique graisseuse de l’enfance. Archives Generales de Medicine 1861 Autographed copy of: De la Paralysie Musculaire Pseudo-hypertrophique1868
Clinical presentation • Delayed walking • Waddling gait • Gower sign • Pelvic muscle weakness and lumbar lordosis • Global developmental delay • Pseudo hypertrophy of muscles • Learning difficulties • Raised CK levels
Duchenne (Xp21) MD • The most common muscle disorder in childhood • X-linked, 30 per 100 000 liveborn males (neonatal screening) • Symptoms appear in first 5 years
Genetics • X linked with recessive inheritance • 1/3 spontaneous mutations • Affects 1 in 3500 live male births • Absence or deficiency of dystrophin in muscle membrane, smooth muscle and brain
Normal DystrophiN Dystrophin Gene dystrophin pre-mRNA dystrophin mRNA DystrophiN protein
Duchenne MD DysX DysXrophin Gene dysxrophin pre-mRNA dysxrophin mRNA DysX protein
Becker MD DysrophiN Dys-rophin Gene dys-rophin pre-mRNA dys-rophin mRNA DysrophiN protein
Surveillance and Treatments in DMD • Heart • Respiratory • Scoliosis • Maintaining ambulation
Respiratory - Problems • Respiratory problems are predictable • Correlation with overall muscle strength and ambulation – rarely problems in ambulant boys • Progressive fall in FVC predicts respiratory failure • Nocturnal hypercapnia – subtle symptoms ie headaches, tiredness, poor performance at school, restless sleep
Respiratory -Problems • Increased amount of chest infections • FVC <40 % indicates sleep studies • Consider flu and pneumococcal vaccination • Early antibiotic treatment • Physio: Postural drainage / assisted cough
What are the symptoms of progressive respiratory failure ? • Subtle • weight loss • reduction in energy levels • poor performance at school. • Sleep disturbance • increased requirement for turning overnight. • Chest infections • frequent and difficult to treat. • Established hypercapnia and not treated • Headaches • general malaise, poor eating • high risk of death from respiratory failure during intercurrent infection.
Evolution of respiratory failure in NMD Surveillance Normal breathing FVC 100% pred Monitor FVC < 60% pred REM related sleep disordered breathing Chest physio FVC < 40% pred NIV Chest infection Cough assist NREM and REM sleep disordered breathing FVC < 20% pred Daytime ventilatory failure Simonds A.
Respiratory Surveillance: • Forced Vital Capacity (FVC) • absolute values and % predicted for height or arm span • easy way to document the progression of respiratory muscle weakness. • FVC drops to 1.25 l or <40% predicted value • serial measurement of overnight oxymetry and CO2 • allows the recognition of the development of nocturnal respiratory failure.
Respiratory- Non-invasive ventilation • Early discussion • Indication: FVC <40 %, nocturnal hypoventilation • Mean age 17 years (Newcastle) • Improvement of daytime symptoms • Less infections • Daytime ventilation later • ? Tolerance
Ventilation- the benefits • Patients notice • frequency of chest infections falls • infections that do occur may be effectively managed with the ventilator to assist coughing. • may develop a need to use the ventilator for increasing periods during the day • a portable ventilator may need to be provided that can be transported on the wheelchair. • Nocturnal ventilation • Long-term follow up studies - very effective as a treatment for respiratory failure • often nocturnal use alone provides very good stabilisation for many years. • Ventilation • mean age of death (Newcastle) 19 years to at least 25 years • survival into the fourth decade is now possible !
Current Respiratory guidelines • ATS Consensus Statement: Respiratory Care of the patient with Duchenne Muscular Dystrophy AJRCCM;2004:456-65 • Recommendation for Respiratory care of children with Spinal Muscular Atrophy Type II & III Neuromusc Disord 2003;13:184-89 • Ventilatory support in Congenital Neuromuscular Disorders – congenital myopathies, congenital muscular dystrophies and SMA II Neuromusc Disord 2004;14:56-69 • MDC Recommendations for the Respiratory care of adults with Muscle Disorders (2005-in preparation) • Consensus Conference: Clin indications for NIV in CRF. Chest 1999;116: 521-4
Are we getting it right ?Incidence and mortality rate for DMD (Denmark) Jeppesen J et al Neuromusc Dis 2003; 13:804-2
Management trends in DMD Jeppesen J Neuromusc Dis 2003;13:804-12
When to initiate NIV in NMD • Background: • NIV can be lifesaving in hypercapnic patients. • Mean survival 9.7 months in hypercapnic DMD patients if ventilatory support not provided (Vianello et al, 1997). • Survival extended in other cohorts (Bach, Eagle, Simonds). • Clinical course in other NMD not so predictable • BUT
Prophylactic NIPPV in DMD Preventative / prophylactic NIV in asymptomatic normocapnic DMD patients is not beneficial Raphael et al Lancet 1994 Control NIV
When to initiate NIV • Initiation of NIV at time of nocturnal hypoventilation before development of daytime hypercapnia will prevent ventilatory decompensation and improve QOL • Initiation of NIV in asymptomatic patients before the onset of sleep disordered breathing or daytime hypercapnia is NOT recommended
How do we compare to others ? European use of ventilation by disease categoriesLloyd Owen ERJ 2005
Cardiac- Surveillance • ECG and ECHO at diagnosis, 2-yearly until 10, yearly thereafter (European Neuromuscular Centre, Netherland) • 10% of female carriers develop overt cardiac failure: ECG and ECHO at diagnosis and 5-yearly
Cardiac -Treatment • Single study suggests ACE inhibitor use before cardiac abnormalities are detectable as protective in the long term • Currently treatment with ACE inhibitors +/- β-blockers is initiated when echo findings of LV dysfunction • Diuretics etc as required for complications
Special case of Emery Dreyfus Muscular Dystrophy • X linked EDMD- arrythmias- pacemaker • AD EDMD- VF-implantable defibrillator
Factors causing loss of ambulation in Duchenne • weakness • contractures progressive scoliosis rapid growth spurt falls/injury /fractures • fear • motivation Marion Main
Ways of maintaining ambulation in NM disorders • maintain power • Steroids in DMD • Beta agonists in SMA • control contractures/deformity • prevent injury • Orthoses • maintain motivation • child and parents/carers Marion Main
Trends in survival in DMD- secular trends Eagle et al Neuromusc Dis 2002
SS= scoliosis surgery Eagle et al Neuromusc Dis 2002
Joint neuro respiratory clinics- doing the right thing ? YES When is the right time to refer to the respiratory team ? EARLY
Advantages of Joint Clinics • Don’t send patient to …x, y, z • Invite …x, y, z, to be part of your team
Who is involved with the care of NM patients? • GP, • community paediatrician at district general hospital • hospital paediatrician at district general hospital, • paediatric neurologist at tertiary hospital, • neuromuscular specialist national centre, • paediatric respiratory consultant and nurse • paediatric cariologist • physiotherapist, • occupational therapist, • speech and language therapist, • dietician, • social worker, • geneticist, • orthotist, • wheelchair services, • orthopaedic surgeon, • spinal surgeon, • neurophysiologist, • Histopathologist, • anaesthetist, • intensivist, • special educational needs teacher. • Neuromuscular nurse specialist • palliative care team • Transitional care team to take over care on reaching adulthood MULTIDISCIPLINARY Parents
The future • What we can do . • What we are trying to do.
What we can do : Role of steroids • Prednisolone / Deflazacort • Regimes: • Prednisolone 0.75 mg/kg/day • Deflazacort 0.9 mg/kg/day • consider alternate day dose or steroid breaks • How long to give it? • Increase in muscle strength • Prolonged ambulation for up to 2 years • ? Improvement in cardiac function • ? Lessen scoliosis • ? Improves respiratory function Cochrane 2004: Improvement in muscle strength and function for 6 months to 2 years