Pacemaker Malfunction
Pacemaker Malfunction. ECG Signs of Pacemaker Malfunction. Failure to output Failure to capture Undersensing Inappropriate pacemaker rate true malfunctions / pseudomalfunctions. Failure to Output. Causes : Oversensing


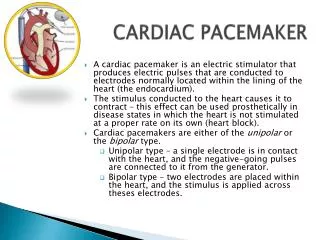
Pacemaker Malfunction
E N D
Presentation Transcript
ECG Signs of Pacemaker Malfunction • Failure to output • Failure to capture • Undersensing • Inappropriate pacemaker rate true malfunctions / pseudomalfunctions
Failure to Output • Causes : • Oversensing • Battery depletion (% of time pacing is required, thresholds necessary, single- or dual-chamber pacing, rate-modulation and other features) • Circuit failure (Lead fracture, disconnection of lead from the PM) • Random component failure (rare) • Pseudomalfunction • Crosstalk (dual-chamber PM) • when the monitor system does not display the pacemaker stimulus artifact when it is really present (frequently with bipolar pacing)
Oversensing • Unexpected sensing of an intracardiac or extracardiac signal. • Intermittent or constant • Electrical signals that may cause oversensing include myopotentials, T waves, and P waves. • Oversensing of myopotentials in a single-chamber PM may result in pauses, whereas oversensing of myopotentials by the atrial-sensing circuit of a dual- chamber PM may result in rapid paced rhythms. • Corrected by reprogramming the sensitivity or by reprogramming the refractory period of the channel on which oversensing is occurring • Oversensing of extracardiac events occurs much less commonly with bipolar sensing.
dual-chamber bipolar PM. Paced ventricular activity is absent after the third paced atrial beat because of oversensing PM programmed to unipolar sensing. Sensing of myopotentials led to symptomatic pauses. Reprogramming the pacemaker to a bipolar sensing prevented myopotential oversensing
Cross talk • Not a true malfunction • In a dual-chamber PM, the PM stimulus in one chamber is sensed in the other chamber. • For the PM-dependent patient, inhibition could result in ventricular asystole. • Most PMs have two methods of protection • Interposition of a short 'blanking period' of refractoriness in the ventricular channel simultaneous with the atrial output stimulus. • Ventricular "safety pacing," whereby any event sensed on the ventricular sensing circuit within a defined early portion of the AV delay initiates the delivery of a ventricular pacing stimulus.
DDD pacemaker. After the third atrial pacing artifact, there is evidence of atrial depolarization, but there is no ventricular pacing output. Failure to deliver the ventricular pacing artifact is due to crosstalk
Failure to Capture • Cause : • Dislodgment of the PM lead from the endocardial surface (usually in the first few weeks) • Break in the insulation of the PM catheter allows some of the current from the electrode to escape into the surrounding tissues. • Impending battery depletion • If the pacing threshold required to depolarize the myocardium is greater than the programmed voltage amplitude and pulse duration (Poor lead position, exit block etc.) • Marked metabolic abnormalities, such as hyperkalemia, and some cardioactive drugs, such as flecainide. • Pseudomalfunction – • Inappropriately low voltage-amplitude and pulse-duration settings • A PM artifact occurring within the myocardial refractory period
DDDR pacemaker. All but one ventricular pacing artifact fail to result in ventricular depolarization, that is, failure to capture Intermittent ventricular failure to capture in a patient with a dual-chamber pacemaker
Undersensing • Intermittent or total • Rarely an urgent problem • Results in PM output that is undesirably competitive with the intrinsic rhythm. • Can result in an unwanted rhythm (eg. atrial pacing that competes with NSR may result in AF). • Competition in the ventricle is possible but is almost never a problem except when the fibrillation threshold has been altered by ischemia, electrolyte imbalance, or some other metabolic abnormality. • Undersensing can frequently be corrected by reprogramming the sensitivity
Causes : • Lead dislodgment • Poor lead position at the time of implantation • Interruption in the insulation of the pacing catheter. • Delivery of a low-amplitude P wave or QRS complex to a normally functioning pacing system. (eg. concomitant drug therapy, body position, MI, and cardiomyopathy) • Pseudomalfunction • Magnet application • Environmental electrical noise • When a P wave or QRS complex falls within the RP of PM • Monitor artifact • In dual-chamber PMs, apparent undersensing may occur during the initial portion of the AV interval (blanking period). During this interval, the ventricular channel of the pacemaker is refractory to avoid sensing of the atrial stimulus and depolarization. If an intrinsic ventricular event occurs during the blanking period, it is not sensed. This problem can be corrected by shortening the blanking period.
ventricular PM programmed to 50 bpm. The second and third pacing artifacts occur inappropriately close to the preceding QRS complex (that is, at less than 1200 ms the programmed rate of the PM) Functional undersensing. ventricular PM programmed to 70 bpm. There is failure to capture with the second and third pacing artifacts. The third pacing stimulus occurs 850 ms after the preceding intrinsic QRS (normal sensing). The fourth pacing stimulus occurs 640 ms after the preceding intrinsic QRS, indicating that the preceding QRS complex was not sensed because it occurred during the pacemaker's ventricular RP
Inappropriate Pacing Rates • Runaway pacemaker • May be lethal for both PM-dependent and non-dependent patients. • Pacing rates may be very rapid and cause hemodynamic instability and collapse. • Result from battery failure, random component failure, or component failure induced by therapeutic radiation. • Treatment is disabling the faulty pacemaker output • Pseudomalfunction Sensing abnormalities • Tracking of atrial fibrillatory or flutter waves • PM re-entrant tachycardia (seen in dual-chamber PMs; occurs when sensing of a retrograde atrial depolarization initiates ventricular pacing, which in turn leads to retrograde conduction and repetition of the cycle). • Electromagnetic interference from the patient's environment may cause the generator to be reset to a rate different from that programmed. • Many PMs operate at a slower rate when battery depletion is imminent.
Pacemaker re-entrant tachycardia with a dual-chamber PM. Atrial and ventricular pacing stimuli precede the first three paced complexes at a rate of 80 bpm. A PVC follows the third paced ventricular complex and is conducted in a retrograde to the atria. The atrial activation is sensed by the PM and initiates ventricular pacing. The pacing rate is limited to the programmed upper rate limit of 110 bpm
Environmental Causes of Pacemaker Malfunction • Electrocautery Causes temporary sensing problems or reprogramming (rarely permanent alteration) • Transthoracic Defibrillation • Can cause reversion to back-up mode, transient increases in capture threshold and loss of capture as well as destruction of the PM generator and circuitry • Damage is minimized by positioning paddles anteroposteriorly and as far from the pacemaker or lead as possible (ideally 15cm). • Extracorporeal Shock-Wave Lithotripsy • Usually synchronized to the patient's ventricular depolarization or to the output stimulus of the PM. • In dual-chamber PMs, synchronization of the lithotriptor with the atrial output can result in inhibition of ventricular output. • In patients with an rate-adaptive PM, sensing of the shock waves can result in increased pacing rates and damage to the piezoelectric crystal. • The following guidelines should be followed : 1) Program the PM to the VVI or VOO mode 2) keep the focal point of the lithotriptor at least 6 inches away
Magnetic Resonance Imaging • All pacemakers to revert to asynchronous mode because of reed-switch closure. • Investigations have shown that MRI does not permanently damage the reed switch or other pulse generator components. • The radiofrequency does not alter the acutely programmed variables, change the normal magnet rate, or induce pacing in most pacemakers tested. • A study by Vahlhaus et al. of 32 patients with PM exposed to MRI at 0.5 Tesla. • Lead impedance, sensing and stimulation thresholds did not change, battery current and impedance tended to increase, no change in programmed data or the ability to interrogate and program. No irreversible changes in PM systems • PACE 2001; 24: 489-95 • In general, MRI should be avoided in a patient with an implanted PM. • MRI may be attempted in non-PM-dependent patients if the device can be programmed to an output at which there is failure to capture or OOO mode. • Low magnetic field (0.5 Tesla) is preferable. • The patient should be monitored by pulse oximetry, blood pressure and ECG • If the body area to be imaged is in close proximity to the PM site, the PM- induced artifact on MRI may obscure the images.
Transcutaneous Electrical Nerve Stimulation • Appears to be safe in most patients with permanent PMs. • It is not known how close to the PM the stimulator can be placed, and it is best to avoid applying the stimulator to a vector or path that would be parallel to the pacing lead. • In patients with VD or DDD PMs, it may result in an increased ventricular rate. • Therapeutic Radiation • Failure of various battery components or accelerated battery depletion • Changes in sensing capability, failure of telemetry function, runaway function and complete shut down may all occur • No specific prediction relative to dose can be made. • Particularly patients undergoing radiation for thoracic / chest wall malignancy. • Precautions - Position the field of radiation at an angle oblique to the PM, total accumulated dosage limit of 2 rad, shielding of the PM with a 1cm margin may be required. • If this is not possible, the PM should be explanted and moved to another site .
RFA • PM should be checked before and after ablation. • Rate response function should be turned off. • RF applications should be as brief as possible and remote from the electrode tip. • If the patient is not dependent, the pacemaker can be programmed to OOO or VVI at a lower rate than the intrinsic heart rate. • If the patient is dependent, the PM should be programmed to VOO mode • Uncommon sources of EMI • dental instruments, including ultrasound scalers and cleaners, and electrosurgical instruments can cause transient inhibition of PM output • Certain cardiac monitoring systems can cause inappropriate rate changes in patients with rate adaptive pacing systems that use a minute ventilation sensor. • Antitheft devices may cause EMI with pacemakers. • Acoustomagnetic systems may cause reversion to asynchronous pacing and rapid ventricular pacing.
Nonmedical Equipment and Devices • Cellular phones • May interact with PM function by inhibiting the pacing output, asynchronous pacing and ventricular triggering. • Hayes DL et al in a multicenter study studied 980 patients. • The incidence of all types of interference was 20%. • Ventricular tracking of signals sensed on the atrial channel, noise reversion and inhibition of ventricular output were the most commonly observed. • The incidence of overall clinical significant interference was 6.6 %. • Interference that was definitely clinically significant occurred in only 1.7 % of tests and only when the phone was held over the pacemaker. • Interference was more common in dual chamber systems (25.3 %) than in single chamber systems (6.8 %) and in digital telephones (24%) compared to analog telephones (3 %). • Patients who are PM dependent should use an analog type cellular phone system. Carrying the phone on the same side of the body as the implanted PM may cause interference. When using the phone, it should be held at least 15 cm away from the PM and on the opposite ear. N Eng J Med 1997; 336: 1473-9
Potentially significant restrictions exist for a small subset of patients who work in environments with equipment capable of causing significant electromagnetic interference— eg. internal combustion engines, arc welding equipment, degaussing equipment and induction ovens. The use of bipolar leads can minimize or eliminate the problem. • Microwaves should not cause any problem. Metal detectors could theoretically cause inhibition of a single beat, but significant clinical sequelae should not result.
Triboelectric simulation • Static electricity or triboelectric phenomena occur more commonly during very cold weather and very low relative humidity. • Triboelectric signals are usually wider and more irregular than pacemaker stimuli • Relatively prolonged overshoot is typical of electrostatic discharge
Pacemaker Syndrome • First described in 1969 by Mitsui et al. • Incidence ranges from 2% to 83%. • Defined as the symptoms associated with right ventricular pacing relieved with the return of A-V and V-V synchrony. • The symptoms include DOE, PND, orthopnea, hypotension, pre-syncope, and syncope. • Additional symptoms include easy fatigability, malaise, headache, and the sensation of fullness and pulsations in the head and neck • Symptoms are most severe when intact V-A conduction is intact. • Signs of congestive heart failure, cannon A-waves.